



Premier Heart’s Multifunction Cardiogram (MCG) Technology Description and Historical Efforts on Phase III/IV Validation Trials over the years.
Solving the most challenging problems in accurate and early diagnosis of heart (and brain) diseases, Joseph T. Shen, a self-taught BioCybernetics Systems Engineer an emancipated physician


Most intellectually honest allopathic cardiologists treating patients with heart failure would acknowledge this reality: more than half of heart failure patients test “normal” on all the costly, potentially deadly, harmful, time-consuming, outdated, and unscalable analog conventional allopathic cardiology tests.
Furthermore, the “diagnosis” of heart failure is often too little and too late. No wonder more people die from heart failure, including younger populations, due to the lack of a proper, accurate early detection diagnostic tool. There is a desperate need for a transformative solution.
For this reason, I have spent half my life developing Premier Heart’s MCG (Multifunction Cardiogram) Technology Platform in a morally responsible, ethical, 100% patient-centered, humanistic, evidence- and empirical data-based, life-saving solution through an unimaginably arduous journey! The good news is that we have successfully brought PH MCG to life, and we are leaving the nightmarish artificial reality brought to you by the corrupt allopathic monopolistic medical-industrial complex.
Premier Heart’s Multifunction Cardiogram Technology justifies its existence by enabling accurate and timely life-saving diagnoses at the bedside in only less than ten minutes, a feat that is impossible with conventional cardiology tools! We have dared to venture into the “Super Domain Intelligence AI” realm when AI was sidelined and in the “AI winter.” Unsurprisingly, industry “experts” regard what MCG delivers as IMPOSSIBLE and INCONCEIVABLE, including the “EXPERTS” IN THE LEGACY CARDIOLOGY. I believe Premier Heart’s MCG represents an exemplary role in leading the transformation, and what we have built is just the beginning of the next industrial revolution.
We are working hard to systematically understand the internal Universe of biological beings physiologically. Our foundational work has successfully created the first RULE-BASED, 100% diligently vetted, strategically chosen, responsible, accountable, moral and ethical empirical evidence-driven safe and effective deep machine learning/Neural Network (AI) digital platform to apply to practical bedside clinical settings anywhere with broadband internet access to aid diagnosis and explore further. Unlike the LLM generative (such as ChatGPT or Google’s Gemini), AI’s tendencies to confabulate and hallucinate at times, our Ruled-Based AI is entirely different from the popular conventional generative AL models in the market. Like Elon Musk, he wants to understand the external Universe around us. He has started building his model. We have successfully built the first biological and physiological beings exploration model to explore our internal Universe and the difference between what we do and what Elon’s team does.

This technology description tells about our work.
Ischemic heart disease, including Coronary artery disease (CAD), is the leading single cause of death in the developed world. Between 15% and 20% of all hospitalizations are the direct results of ischemia from multiple causes and lead to an estimated 23 million people dying annually. The record denotes that the industry captured arrogant, pompous, monopolistic, irresponsible, unaccountable, profit-driven, pseudoscientific, dishonest, baseless, fraudulent, and unsalable analog 19th-century allopathic Cardiology has a failed legacy.

Electrocardiography-(EKG)-based methods, now 125 years old and ossified, are still routinely used as the first initial screening and diagnosis tools. However, our database accumulated over the decades has shown that their accuracy rates are around 13-15% in detecting obstructive coronary artery disease (CAD), not to mention misdiagnosing other essential conditions, including, but not limited to, metabolic heart dysfunctions, cardiomyopathy, myocardial inflammation/myocarditis, and often and frequently misdiagnosed causes of heart failure, etc. We have learned these facts through years of studies based on Premier Heart’s extensive real-world datasets, which we have accumulated over the decades. This discovery revealed two startling facts:
No one, especially throughout the legacy cross-generations of the academic echo chambers, obliviously had questioned or investigated whether ECG truly worked as intended in its 125-year history until we started deeply investigating the real-world data to justify the need for a better and valuable new system.
The EKG industry, supported by academics (or the so-called thought leaders) in corrupt pay-to-play academic echo chambers, is an institutionally normalized scam, a disgusting “Kabuki Dance Theater” of captured and paid soulless academic mouthpieces.
We have also thoroughly investigated the sensitivity and specificity of stress test methods, such as a combination of stress echo, nuclear imaging, and pharmacological tests. Collectively, these methods demonstrate an accuracy of less than 50%! These methods are minimally effective and pose safety concerns, especially in single-vessel CAD cases. They generated two-thirds of the false positive results, leading to unnecessary coronary angiograms and interventions.
Coronary angiography and CTA remain the gold standard for the diagnosis of “Obstructive Coronary Artery disease” to seek profitable coronary interventions during the same procedure, with dubious patient benefits. And evidence has proven that the entire interventional cardiology enterprise is resource-intensive, time-consuming, unscalable, expensive, invasive, and bears a relevant procedure-related complication rate (< 2%), morbidity (0.03-0.25%), and mortality (0.01-0.05%). Additionally, coronary interventions such as PTCA/Stenting or coronary bypass surgeries have repeatedly proven ineffective and deliver little or no benefits for patients with chronic CAD at all when compared to conservative medical management. Furthermore, legacy medical and interventional paradigms of the American Allopathic Cardiology produce unacceptably high Major Adverse Cardiac Events, also known as MACE, in the real world, leading to unacceptable premature deaths and injuries due to a lack of fundamental understanding of the physiological reasoning behind the pathologies.
The hallmark of the failed legacy of allopathic cardiology is a fundamental lack of innovation in a much-needed safe, effective, accurate, and scalable non-invasive “do-no-harm” bedside tool to DETECT signs of physiological dysfunction in their EARLY stages to enable effective disease reversal and timely prevention. All conventional diagnostic tools detect late-stage diseases, with many treatments often being too little and too late. These legacy phenomena are emblematic of the decades-long systematic technological stagnation of a corrupt, ossified, and obsolete system Peter Thiel has written about and lamented for years. We have witnessed and investigated the phenomena firsthand! Unfortunately, Peter has been correct all along.
Premier Heart’s Multifunction Cardiogram (MCG) fundamentally solves this problem and leads medicine into the 21st Century! The future of medicine is with the paradigm of early detection and monitoring of the signs of physiological dysfunctions from the earliest to the latest stages to discover the root causes to prevent and reverse the progression of the disease process, primarily through learning to live an optimal healthier lifestyle, in a cleaner environment, eat healthier wholesome, nutritious foods devoid of ultra-processed foods and toxic chemicals, thus to extend a healthier lifespan and ultimately save lives.
Premier Heart’s Multifunction Cardiogram (MCG) is an entirely new approach to diagnosing metabolic heart diseases, including myocardial ischemia, caused by many root causes of supply and demand imbalances, including but not ONLY limited to coronary heart disease. Following decades of research and development, through the diligent work of two generations of dedicated scientists, clinicians, and engineers, MCG technology has successfully demonstrated its capability in the detection of myocardial ischemia caused by obstructive coronary disease (CAD) in multiple independently conducted clinical validation trials with high sensitivity (89-100%), specificity (83-94%), and accuracy (90 to 100%). We have initiated building a prominent decentralized distributed data registry of millions worldwide to explore the root causes of myocardial ischemia and other non-ischemic pathologies in-depth, with continuous sustained efforts to grow the algorithm’s sophistication and discover new modeling, verification, and validation for the future versions into the 22nd Century and beyond.
The McG model provides characterization for at least 26 pathological and physiopathological conditions, helping to address the lack of accurate detection of myocardial ischemia caused by coronary artery disease and other non-ischemic pathologies, as well as difficult-to-diagnose conditions such as cardiomyopathy and myocarditis.
Theoretical Foundation:
Einthoven historically presumed the myocardium to be a single-point electrical generator emitting vectors three-dimensionally into infinity. Unfortunately, after 125 years, our in-depth studies have concluded that the Einthoven hypothesis has NEVER worked to deliver the intended effectiveness in detecting and quantifying heart disease. All the technologies built based on Einthoven's ossified theory have never delivered the clinical usefulness clinicians need to be effective diagnosticians. This rationale gives us the basis for researching and developing Premier Heart's MCG technology.
To transform the industry, our research leading to the development of Premier Heart's MCG began by using a mathematical description of two core physiologic properties of the heart:
First, the myocardium is a viscoelastic solid via the LaGrange Coordinate.
Second, blood is a non-Newtonian fluid at low and intermediate shearing states via the Eüler Coordinate.
We adopted the “Laplace transform” to fuse these two coordinates into one major mathematical complex, the “LaGrange-Eüler” Equation, which guides our system’s technology development history.
We also adopted Professor NobeWeiner’s “Control Theory” and or his “Cybernetic Systems Mathematical Principals,” combined with the “LaGrange-Eüler Equation,” as our systems technology design guiding compass pointing to the magnetic north, which states that one can extract the unprecedented and vast amount of system internal functional information physiologically from the communications between an input (Lead V5) and an output (Lead II) or vice versa, to understand how the targeted system functions fully. Our work has proven that Professor Weiner's ground-breaking theory works as envisioned. We are honored to be the first to deliver the definitive proof.
The Data collection and reporting process:

Quinquinquagintillion equals the sum of Google (1x10 to the 100th power) plus the number of visible atoms in the entire Universe (1x10 to the 68th power). It also equals approximately 10x the human body's 70K to 100K trillion mitochondria as its biological energy/power grid! Imagine how spectacular this discovery truly is!!!
The mitochondrial network drives ALL cellular energy needs, immediately and profoundly impacting cellular survival. Thus, the delicate energetic requirements of the AMPK master switch depend on the balance of the mitochondria in each cell. Furthermore, scientists have demonstrated that a mitochondrial pool of AMPK is present in multiple tissues and consists of distinct isoforms that are conserved between mice and humans. The direct, localized, physical link between mitochondria and AMPK signifies the mitochondrial network's vital role in maintaining cellular energy for survival.
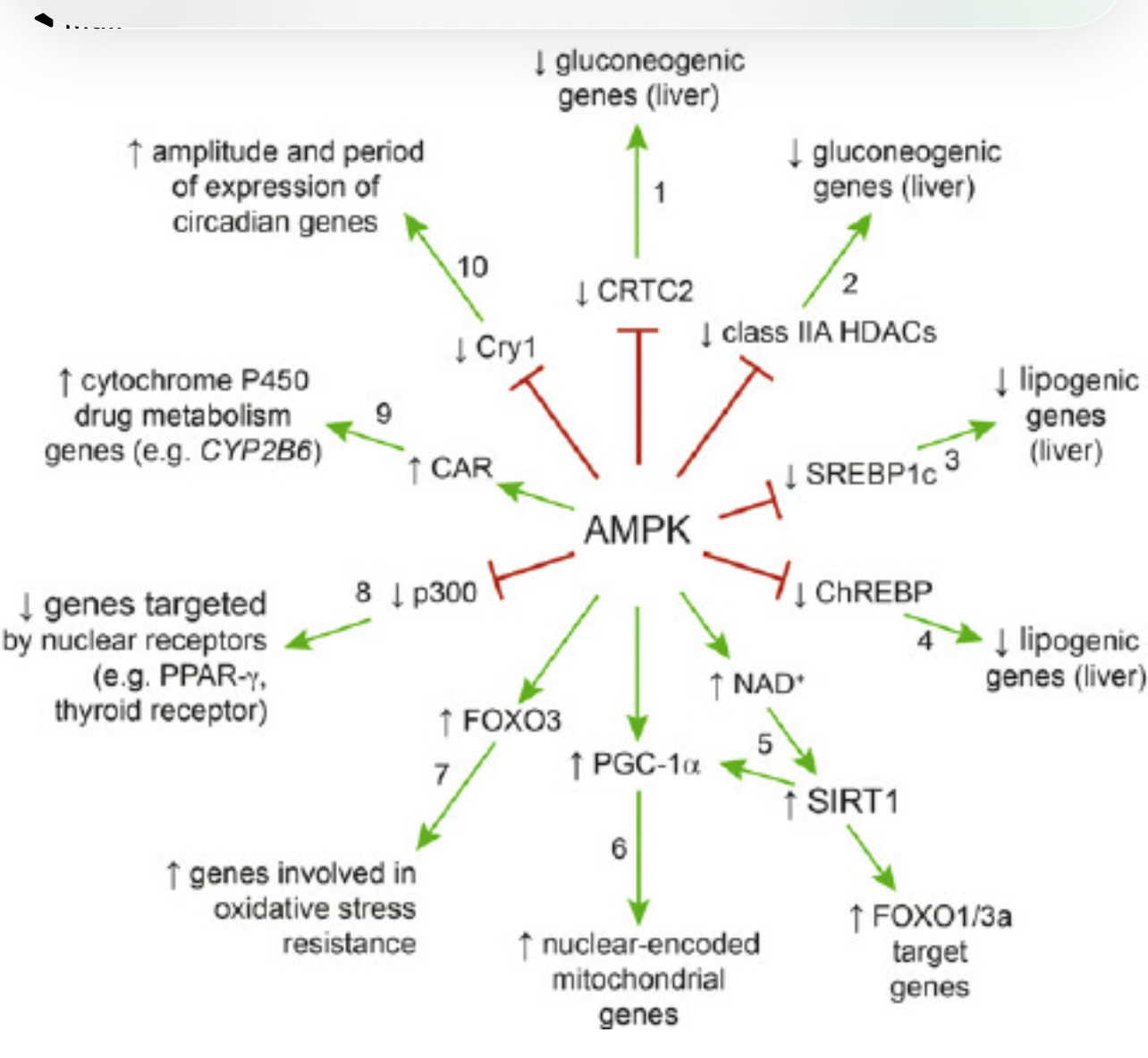
The AMPK Switch Pathway is unique. It remains a master metabolic and genetic survival switch throughout our lives. Diet, exercise, intermittent fasting, caloric restriction, and every medicine that reduces cardiovascular events more than it lowers the target risk factor activate AMPK. Fatty liver, excessive visceral fat, and uncontrolled hyperinsulinemia (thus, the mTOR pathway is switched on, and AMPK is switched off) due to frequent eating, obesity, alcoholism, tobacco smoking, etc., will cause chronic disease and early death. We measure and monitor the balance between the mTOR and AMPK pathways for the cellular aging/death and rejuvenation/survival processes in near real-time throughout the lifetime. The patient's portable device automatically records 4 to 5 82-second cycles of complete resting ECG analog signals from leads II and V5. The recorded signals are then digitized, encrypted, and securely transmitted, along with the patient’s demographic information, to a central data center for processing.
We have built the first deep learning platform in human knowledge of physiology to usher in a RULE_BASED, clean, and vetted empirical data, responsible, honest internal and external verification, validation, replication, and reproducing the results to ensure 100% fidelity and deliver the highest possible accuracy. The goal is to detect physiological dysfunctions early for early prevention and disease reversal and assist clinicians in providing the best possible outcomes for the lowest possible costs so people can live healthier and longer lives.

We perform Discrete Fast Fourier Transformations on the acquired analog ECG data, transforming the analog signals into digital format. Then, we apply signal averaging to deliver the high-quality 82-second digitized signal segments for further transformations.
In the next step, we apply the Systems theory mathematical models based on the LaGrange-Eüler theory. We combine the results of six (6) mathematical transformations* (coherence, phase angle shift, impulse response, cross-correlation, transfer function, and amplitude histogram) based on the auto-power spectra from the recorded ECG leads.
These six mathematical transformations (12 phases) supply unprecedented aspects of the heart muscles’ electrophysiological and mathematical properties concerning blood flow, physiological properties, and impact on myocardial functions. The MCG technology is similar to the unprecedented new information the James Webb Space Telescope discovered in the deep Universe! The information we deliver concerning the heart and brain is invisible or non-existent in the conventional legacy allopathic world.
Ironically, industry experts with rudimentary knowledge of our technological advances believe that what we have built is inconceivable and impossible. They further insist that technology like ours will not be possible until 2050 or beyond. They pretend that we do not exist, and worse yet, they have tried to censor and delete us; imagine that!
All these functions produce the post-DSP 168 empirically derived mathematical elements, allowing the discoveries of vast (10 to the 168th power) parameters over the decades. The patterns of the parameters from a patient match similar patterns obtained from over 250,000 individuals (men and women, 50% each), of whom 60% had various degrees of CAD (including status and severity) confirmed by coronary angiography, including FFR, Classical and Functional Syntax Scores, the platinum standards of interventional cardiology. The data procurement to clean, vet, and data, then train, verify, and validate our neuro network diagnostic algorithms to ensure the safety, accuracy, and effectiveness of the platform, have taken us decades to achieve due to the inaccurate fragmented diagnosis with a wrong focus on the surface phenomenon, such as the descriptive terms such as the “obstructive coronary artery disease,” atrial fibrillation,” etc., rather than finding the root causes of the clinical presentations, and unscalable nature of the legacy medicine world.
The MCG pattern of each test has been validated and correlated with the presence/absence and severity of CAD, ranging from as little as 30% single-vessel disease to 100% occluded coronaries with or without the collateral circulation formations (self-healing of the heart) and other invisible conditions of the coronary supply and demand imbalances physiologically, impossible in the conventional legacy analog world.
The database also contains results of the patients having:
Clinically Normal people ages 14 to 100
50/50 male/female ratio
No evidence of visible CAD
cardiac ischemia disease
one or more non-ischemic cardiac diseases
both cardiac ischemia and non-ischemic cardiac disease(s)
many forms of heart diseases (e.g., arrhythmias, hypertrophy, cardiomyopathy) with or without CAD
Clinical studies have shown that MCG™ is sensitive to 90 to 100%, with 0 to 7% false negative results, and specific to 85 to 99%, with 1 to 15% false positive results, in detecting ischemia due to coronary artery disease (CAD). However, patients with adequate collateral circulation may test low or normal on MCG. Cardiologists may label these patients as false negative cases. On the other hand, patients who have NO Visible CAD can have very high ischemia and other abnormal expressions on MCG due to many root causes (see below). Cardiologists may falsely label these cases as false positive cases.
In addition, due to our deep understanding of creating AI applications and the potential pitfalls. Another important aspect of our work is that we separate the Production environment and the Development environment to ensure safety and effectiveness without endangering our customers and those they serve:
The Development Environment:
Our development environment is an open neural network deep learning environment. We allow developers to reach far and wide to ensure that the learning is complete without hindrance. We are adding additional learning layers and wide-ranging data input to optimize learning. This environment allows maximum creativity to flourish and grow. Once we are satisfied with an application and responsibly implement a “locked down “version, we will move it to the production side.
The production environment:
The production platform is a ruled-based, empirical-data-based, LOCKED DOWN system. We repeatedly optimize, automate, and validate the customer-facing production version of our analysis engine internally and externally until we are convinced that the application works as intended without any hallucinations or falsified reporting. Then, we lock it down and launch it for commercial applications. Every version update goes through the same process.
ISCHEMIA RESULTS and the MCG SEVERITY SCORES:
Note: when encountering alternating global/local/borderline/no ischemia patterns, one must consider the possibilities of functional ischemia. Shockingly, in reality, the ALMIGHTY “obstructive coronary ischemia” does NOT rank first on the differential diagnosis list, certainly not the NUMBER ONE differential diagnosis at all. We now know that coronary interventions, such as PTCA, Stenting, and the Coronary Bypass Artery Grafting (CABG) procedure, produce zero clinical benefits to patients diagnosed with chronic coronary artery disease. One must consider the rationale behind referring a patient to undergo such procedures.
Word of Caution: Thanks to our decades of dedicated, shoestring budgets but determined, meticulous empirical data mining to train your neuro-network, we have discovered and defined the digital parameters of 1x10 to 168th power, or “Q" inquinquagintillion” “o digitally mirror the biological mitochondrial network system (containing 10 x of ~ 70K to ~100k trillion mitochondria) of the human heart and brain. MCG detects, quantifies, and monitors myocardial ischemia or cellular quiescence as a result of ANY cause that leads to supply and demand imbalances physiologically, including but not limited to mitochondrial dysfunctions due to the following partial list of differentials:
Anemia (Invisible)
Hypoxia (Invisible)
Hypoxemia (Invisible)
Hyperinsulinemia, central obesity (particularly too much belly or visceral fat, fatty liver), and overweight due to overeating/snacking (Invisible, blind-sighted)
Insulin resistance (Invisible), early-stage Diabetes, metabolic dysfunction
Diabetes (Invisible)
Overweight and Obesity (Invisible)
Nutrient deficiencies (Invisible)
Poor sedentary lifestyles (Invisible)
Women's Heart Dysfunctions due to pre-eclampsia, eclampsia, polycystic ovarian disease, Broken Heart Syndrome, Insulin Resistance, Obesity, etc. (Invisible)
Maternal-fetal, Pediatrics, and Adolescent Preventive lifestyle medicine applications (current aims of development)
Environmental toxins such as heavy metals, insecticides, pesticides, and herbicides (Invisible)
Eating ultra-processed foods such as seed oils, sugar, flours, alcohol, etc., (Invisible)
Fatty liver disease (Alcohol or non-alcohol) and excessive belly fat
Tobacco smoking (Invisible)
Air pollution (Invisible)
Narcotics, such as Fentanyl, Cocaine (Invisible)
The Effects of Cyanide (Invisible)
Any root cause leading to all stages of heart failure (Invisible)
Coronary artery disease, early stages, non-obstructive types (hardly visible)
Endothelial dysfunction (Invisible)
Microvascular disease (Invisible)
Neuroendocrine disorders (Invisible)
Acute or chronic exposure to stress (Invisible)
Thyroid dysfunction (Invisible)
Autoimmune disorders (Invisible)
Prescription medications, fitness programs, and supplements (Invisible)
Impact of, or lack thereof, implantable medical devices (Invisible)
Impact of cancer and treatment options, such as chemotherapy, radiation, immunological bone marrow transplants, etc. (Invisible)
Religious rituals or lifestyle choices such as fasting and intermittent fasting (Invisible)
Impact of treatment guidelines from alphabet medical institutions, or lack thereof (Invisible)
Medical Society AMA CPT Code recommendations, Insurance companies coverage policies (Invisible)
Impact of socioeconomic status (Invisible)
Effects of poorly administered general anesthesia (Invisible)
High-altitude sickness (Invisible)
Deep-sea-diving accidents (the Bends) (Invisible)
Space travelers’ physiological effects on humans and animals (Invisible but very useful)
The physiological impact of Space travel (Invisible)
coronary angiogram visible obstructive coronary artery disease of varying degrees (less than 15% in our database).
Any root causes disrupting normal mTOR, AMPK, and cellular autophagy functions (Invisible)
Type I, II, III, IV, and V Diabetes.
Thus, please do not regard conditions that are invisible to the naked eye (any vessel less than 7mm on an angiogram) as false positive cases that could misdiagnose patients’ conditions. Clinicians, please explore the patient's journey and find the root cause to save your patients! Please do not irresponsibly lump your patients into a “Syndrom-X” bucket and abandon them. You are their last hope for survival, doctors! Instead of wittingly or unwittingly becoming drugs, devices, and procedures salespeople, now you can apply real-world empirical evidence and physiology knowledge to make decisions in the best interests of your patients and become the genuine healers you have spent your lives to become!
I have decided to post the article link below describing how people can use it as a basis to interpret their own MCG reports:
Interpreting an MCG Report

Before we dive into the specifics, I’d like to make the following statements:
Global ischemia refers to ischemia of the entire heart, whereas local ischemia refers to partial heart involvement, nothing more or less.
As you can see, legacy allopathic cardiologists are flying blindfolded without knowing their best diagnostic tools for merely detecting incoherent patches of the tip of the iceberg of all the possible physiological dysfunctions of the cardiometabolic system and its environment. They are missing the majority of the metabolic, immunological, environmental, pharmacological, dietary, sedentary lifestyle, etc., as root causes of heart attacks and heart failure. Please share this blog post with everyone, especially your cardiologist if you know one.
The following tables illustrate the shortcomings and the urgent need for the fundamental transformation we bring to the table:
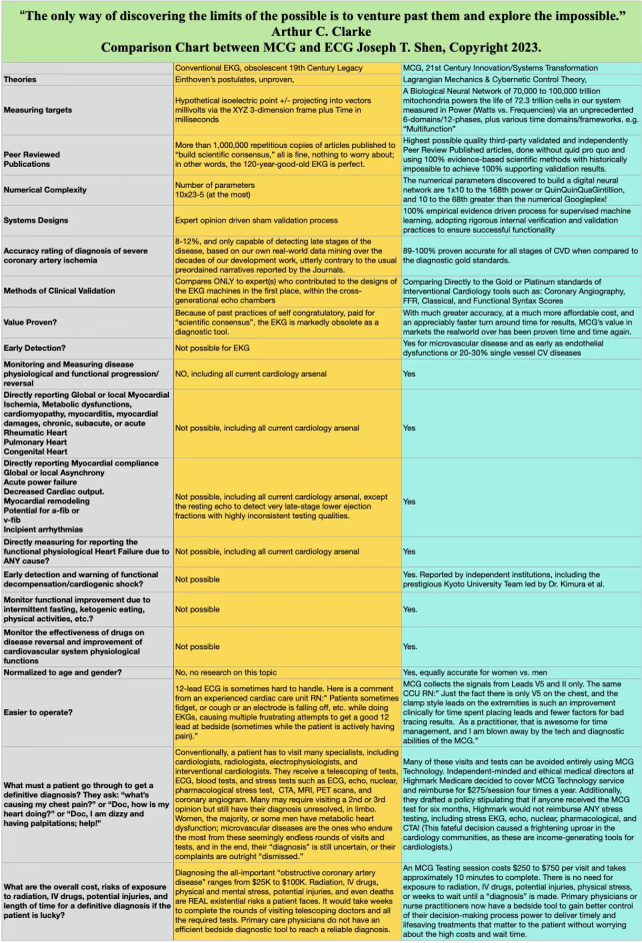

Here are some examples of how we help people with metabolic dysfunctions impacting their hearts:
And our journey to validate our claims in real-world clinical settings through blinded independent cream-of-the-crop ethical volunteering investigators without any industry standard pay-to-pay or corrupt quid pro quo:
The Journey to Freedom of an emancipated enslaved physician

Edited and updated version of the Chapter 12 Multifunction Cardiogram, a.k.a. MCG Technology, Mark Houston’s “Personalized and Precision Integrative Cardiovascular Medicine” 1st Edition Joseph Shen, MD, Raffi Bianchi Shen (Editor),
Please see my response to a major insurance company's senior medical director about how I believe there is a right and best way to evaluate a diagnostic test or a drug.
“H”, Dr. Xxxx; we all know that nearly 90% of the published data by the academic literature and guidelines made through medical societies, CMS, ICER, and other well-established organizations are flawed and based on pseudoscientific key opinion leaders” pinions rather than ethically and morally collected transparently 💯 % objective empirical data without the corrupt “c" erry-picked data sets” “o fit the preordained narratives and deliver predetermined outcomes. I believe that this colossal systemic corruption is the root cause of the out-of-control chronic diseases in America.
Thus, I recommend that your group look beyond the conventional legacy and use real-world empirical evidence and the scientific method to evaluate the work we have consistently done to build our technology platform. Thank you!
His reaction has been positive thus far. We shall see if they will ultimately surrender to bring themselves to the right decision!
Finally, it is heartwarming to witness the cultural shift toward what we have been working on - rethinking and redesigning the legacy of the American Medical system's corrupt and ossified dumpster fire since the 1990s to build a new system everyone deserves.
Our future is bright:
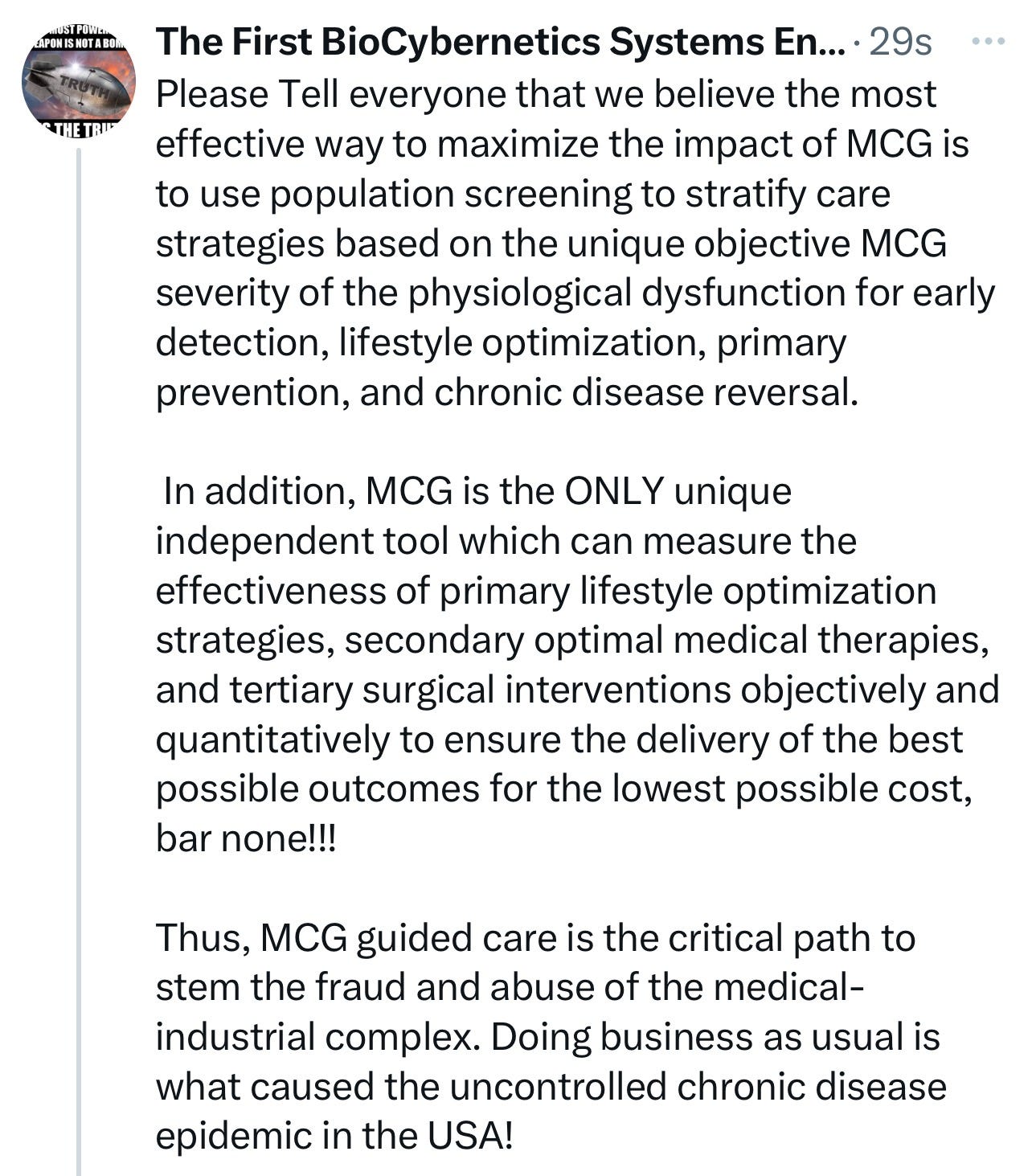
We are creating a people-centric computational electrophysiology world sporting an individually owned, vetted, and monetized decentralized data network managed via a blockchain ledger to ensure fidelity, honesty, and ethical standards in how our health data is used for deeper machine learning. The goal is to improve care for the best possible outcomes at the lowest possible cost for everyone. There will be no middlemen in this system. Our users will verify and validate any diagnostic criteria, drugs, supplements, devices, procedures, insurance coverage policies, clinical guidelines, peer-reviewed studies, and legislation to independently determine their fundamental values without the corrupt pay-to-play quid pro quo, cherry-picking the data to fit preordained narratives to deliver the predetermined outcomes. The system will assess anyone who contributes and analyzes the data to this new “keeping every" ne honest” network and “ill be judged based on merits and ability to deliver.
Our b2c direct personal monitoring devices will spearhead the formation of this robust data network for 21st-century healthcare delivery.
We must no longer allow corrupt operators to access people’s data to gaslight and manipulate them diabolically, ultimately plundering them. There is no need to lie for profit; people will make a decent living by telling the truth and delivering their best work.
Enough! Time to move on and move forward with us!
Joseph
Joseph T. Shen, the first BioCybernetics Systems Engineer
As Sir. Arthur C. Clarke once said, "The only way to truly understand the limits of the possible is to push past them and explore the impossible.”
This philosophy guides our work at MCG, where we constantly push the boundaries of what is achievable in bioengineering and technology.
I am an independent, emancipated, fully recovered, rebellious physician who stands for personal freedom and sovereignty. In 1998, I became a self-taught pioneer in bio-cybernetic systems and information technology engineering. With my deep knowledge of how the legacy of allopathic medicine was a dumpster fire of “artificial reality” that gaslit, scammed, and plundered the unsuspecting masses. From thereon, I have focused on developing computational bio-cybernetics, Lagrangian mechanics systems, and deep machine learning of heart- and brain-saving intelligent technologies. I have never looked back!
Researcher and Technology Developer
Managing Member
Premier Heart, LLC
Premier Heart International, LLC
Premier Heart Japan, Inc.
Emergency MCG USA, Inc.
110 Main Street, Suite 201-88
Port Washington, NY 11050
Tel: 516-883-3383 ex 8102
Fax: 516-883-5812
Mobile: 516-603-6368 (Please alert me who you are with a text message first; please do not respond to unknown numbers. I WILL respond as soon as possible.)
Email: jtshenmd@premierheart.com (mailto:jtshenmd@premierheart.com)