

Interpreting an MCG Report
Why Premier Heart's MCG will revolutionize the way people see and do healthcare.

Before we dive into the specifics, I’d like to make the following statements:
The core issue with traditional allopathic cardiology is its lack of innovation in developing a reliable and objective bedside tool to detect early signs of physiological issues beyond all the legacy diagnostic tests of the 20th Century. Such an objective, accurate, and early detection tool would allow for effective disease reversal and prevention. Currently, most diagnostic methods identify diseases only at advanced later stages, often making treatments insufficient or too late. These longstanding problems highlight decades of technological stagnation within a system that has become corrupt, ossified, and outdated, as Peter Thiel has criticized for years. We have directly observed and studied these issues, and Thiel's assessments have proven correct.
We developed technology to accomplish a long-overdue, and desperately needed, primary goal: building a super-domain-intelligent, deep-machine/human-learning, computational systems engineering approach that extracts objective, fundamental physiological data from the heart and brain, both qualitatively and quantitatively. This aims to enhance bedside diagnoses for greater accuracy once and for all. The reason we did not adopt large language models (LLMs) in the current “AI races” is that we have learned from IBM’s failure. IBM created 'IBM Watson Health” with multi-billion dollar efforts to improve cancer diagnosis and treatment by reading published legacy “medical literature” without recognizing how flawed and corrupted that literature is—nearly 90% of it is based on medical-industrial complex captured “expert opinions” to promote their preordained narratives and pre-decided outcomes, rather than objective data. Unfortunately, IBM Watson’s tragic failure became a classic example of “garbage-in, garbage-out.” Coupled with LLMs’ AI tendency to hallucinate and the deeply flawed, corrupted source material from legacy literature, IBM Watson Health was doomed to fail, as we predicted.
Our technology will serve as the core infrastructure of a new 21st-century system centered on patient-specific diagnostic decision-making, where objective mathematical truths about an individual's overall physiological performance are supported by reliable real-world clinical historical data. We assess treatment options using objective, math-based criteria, not influenced by incentives from the medical industry. In this new landscape, any treatment will be evaluated based on its outcomes and cost-effectiveness to determine if it is worthwhile.
Premier Heart’s Multifunction Cardiogram (MCG) TM fundamentally addresses the systemic lack of accurate, reliable, safe, trustworthy, and effective bedside diagnostic tools for frontline clinicians serving the population daily under a failing legacy system. Premier Heart, LLC leads medicine into the 21st century and beyond! The future of medicine emphasizes early detection and monitoring of physiological dysfunctions from the earliest to the latest stages to identify root causes, prevent and reverse disease progression, mainly through adopting a healthier lifestyle, living in a cleaner environment, and eating wholesome, nutritious foods free from lifelong dependence on prescription drugs.
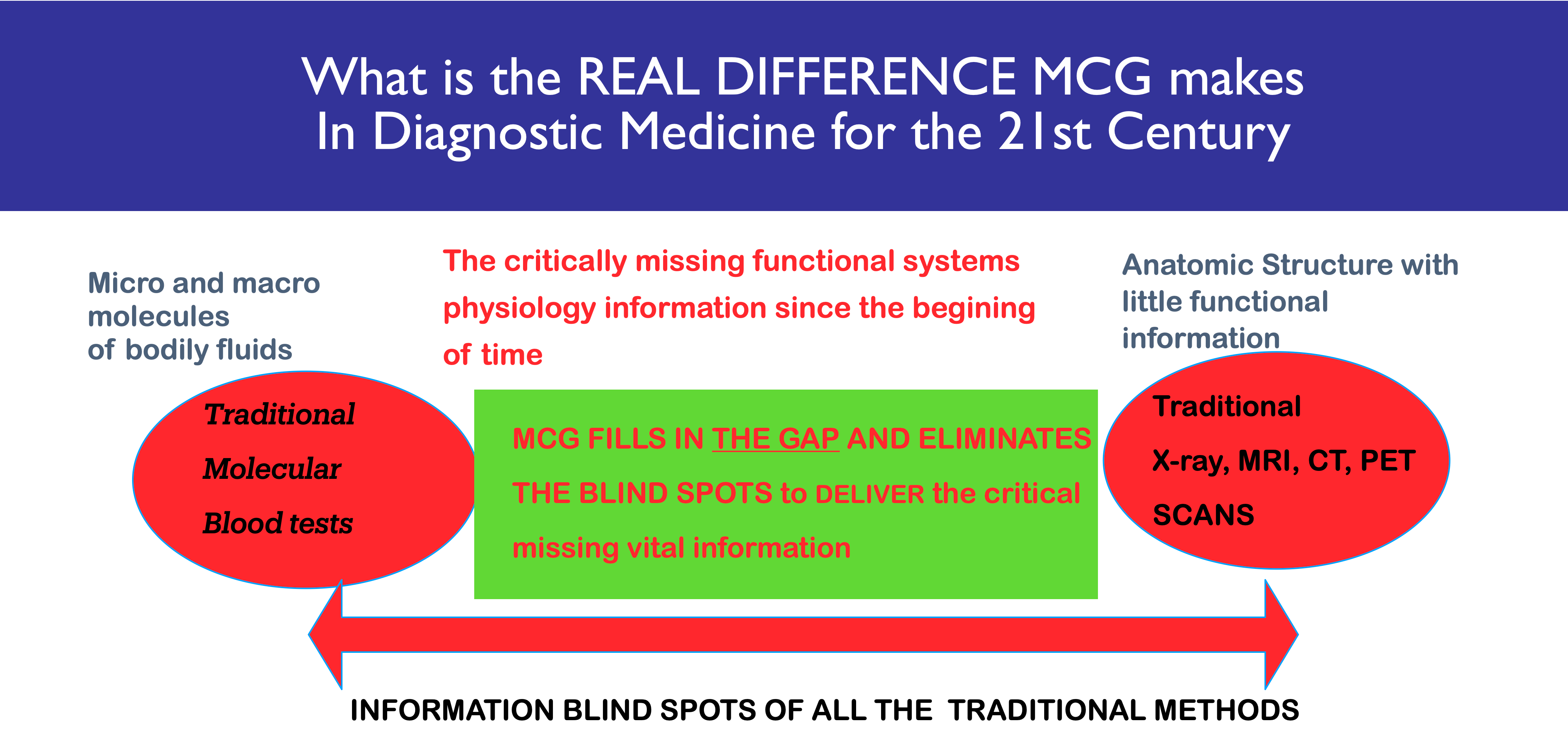
MCG Fills the Gap and Blind Spots Missing in the Allopathic Diagnostic Technology Arsenal.
Before we dive into the specifics of how to read and interpret an MCG report, I encourage everyone to watch and share the podcasts I created recently to enhance your learning and understanding of what and why we do MCG:


Let’s begin.
MCG TEST RESULTS ANALYSIS

ISCHEMIA RESULTS and the MCG SEVERITY SCORES:
Word of Caution: Thanks to our decades of dedicated, on shoestring budgets, but determined, meticulous empirical data mining to train the world’s first empirical evidence, objective, and reality-based, founded on a set of immutable, objective truth, and immortal mathematical principals, 100% empirical evidence-driven, and patient-benefit-centric deep machine learning neuro-network to aid diagnosis of heart and brain physiological dysfunctions, with a laser-focus on the biological mitochondrial networks as a system, its dysfunctions leading to chronic (and acute) diseases, we have discovered and defined the digital parameters of 1x10 to 168th power, “Quinquinquagintillion” to mirror the biological mitochondrial system’s (containing 10 x of approximate 70K to 100k trillion mitochondria) of the functioning human heart and brain. MCG detects, quantifies, and monitors myocardial Ischemia or cellular quiescence as a result of ANY cause that leads to supply and demand imbalances physiologically, including but not limited to mitochondrial dysfunctions due to anemia, hypoxia, hypoxemia, insulin resistance, Diabetes, nutrient deficiencies, poor sedentary, stressful lifestyles, environmental toxins such as heavy metals, insecticide, pesticides, eating ultra-processed “foods” such as seed oils, sugar, flours, Alcohol, etc., tobacco smoking, air pollution, narcotics, such as Fentanyl, Cocaine, the effects of Cynide, environmental toxins, any root causes disrupting mTOR, AMPK pathways’ normal functions, any root cause leading to all stages of heart failure, coronary artery disease, endothelial dysfunction, microvascular disease, neuroendocrine disorders, acute or chronic exposures to stress, Thyroid dysfunction, medications, general anesthesia, high-altitude-sickness, deep-sea-diving accidents (the Bends), and coronary angiogram visible obstructive coronary artery disease (less than 15% in our database). Thus, do not treat the conditions MCG reported as “invisible” (any vessel less than 7mm on their angiogram) to the naked eyes of interventional cardiologists as “false positive” cases to misdiagnose patients’ conditions. These are the blind spots which lead to misdiagnosis and harm to your patients. Thus, clinicians, please explore the information, help your patients on their journey, and strive to find the root cause(s) to save them! Please do not irresponsibly lump your patients into a “Syndrome X” bucket of “No-Men’s-Land” and abandon them. You are their last hope for survival, doctors!
It is critical to understand that we created this report to allow clinicians and their patients to read the output using the language they are accustomed to, except for a few pathophysiological conditions, such as incipient arrhythmias, myocardial compliance, and synchronization, which are unique to our technology. Nevertheless, these “foreign” terms, unavailable in the legacy cardiology conventional reporting, are clinically advantageous to denote how the targeted heart functions to save lives.
Global Ischemia denotes Ischemia of the entire heart, whereas local Ischemia denotes partial heart involvement, nothing more.
Note: when encountering alternating global/local/borderline/none ischemia patterns, one must consider the possibilities of “functional ischemia.” Shockingly, the ALMIGHTY “obstructive coronary ischemia” is NOT the first on the differential diagnosis list, certainly not the NUMBER ONE differential diagnosis at all. We now know that coronary interventions, such as PTCA, Stenting, and the Coronary Bypass Artery Grafting (CABG) procedure, produce zero clinical benefits to patients diagnosed with chronic coronary artery disease. One must consider the rationale behind referring a patient to undergo such procedures.
The eight category icons in the report are self-explanatory.
We build MCG on the promise that the technology can and should detect the earliest possible abnormal cardiovascular energy production biological network (i.e., the biological mitochondrial network), which functions for timely lifestyle reversal and disease prevention. MCG is the only test that could deliver that information.
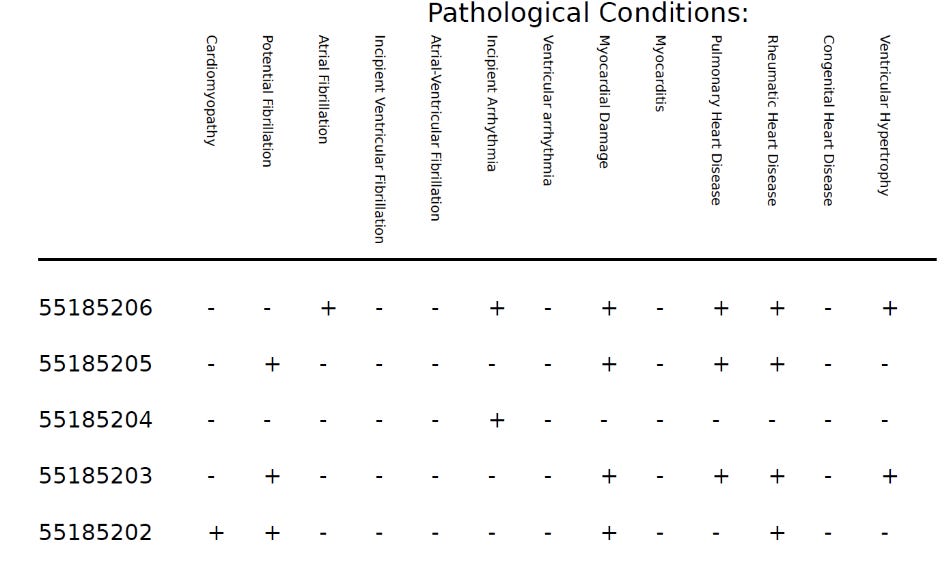
PATHOLOGICAL CONDITIONS: (For clinicians’ references and pattern recognition purposes only, not definitive diagnosis)
Cardiomyopathy:
Cardiomyopathy (kahr-dio-my-OP-uh-thee) is a disease of the heart muscle. It causes the heart to have a more challenging time pumping blood to the rest of the body, leading to heart failure symptoms. There are various types of cardiomyopathy. The main types include dilated, hypertrophic, congenital or acquired HOCM, and restrictive cardiomyopathy, among others.
Potential Fibrillation:
These are potentials of small amplitude and brief time frames resulting from a single heart muscle fiber, undetectable by the conventional EKG. Their rhythmicity and morphology identify them as fibrillations. Each potential appears the same, suggesting the same heart fiber discharges the same fiber repetitively. These findings are unique to MCG and impossible for ANY conventional legacy tools to detect.
Atrial Fibrillation:
Atrial fibrillation (A-fib) is an irregular heart rhythm that begins in your heart's upper chambers (atria). Symptoms include fatigue, heart palpitations, shortness of breath, and dizziness. A-fib is one of the most common arrhythmias. MCG detects A-fib unconventionally and A-fib unconventionally and thus can, at times, detect when the conventional EKG fails to detect.
Incipient Ventricular Fibrillation: (Initial early stage)
Ventricular fibrillation is a type of irregular heart rhythm (Arrhythmia). During ventricular fibrillation, the lower heart chambers contract in a very rapid and uncoordinated manner. As a result, the heart doesn't pump blood to the rest of the body.
Ventricular fibrillation may require immediate medical attention. It's the most frequent cause of sudden cardiac death.
MCG detects V-fib unconventionally, so it can detect it when the traditional EKG fails to do so. Thus, it can detect it when the conventional EKG fails to detect it, so it can detect it when the traditional EKG fails to.
Atrial-Ventricular Fibrillation:
Atrial fibrillation (A-Fib) and ventricular fibrillation (V-Fib) are both types of irregular heartbeats or arrhythmias that can be serious. A-Fib affects the upper chambers, while V-Fib affects the lower chambers. Both conditions can cause an irregular and often fast heart rate, but V-Fib can be more dangerous and immediately life-threatening.
MCG detects A-fib/V-fib combination uniquely and unconventionally, thus can detect when the conventional EKG fails to detect.
Incipient Arrhythmia: (Early stages)
An arrhythmia, or irregular heartbeat, is a problem with the rate or rhythm of your heartbeat. Your heart may beat too quickly, too slowly, or with an irregular rhythm. One expects your heart rate to speed up during physical activity and to slow down while resting or sleeping.
MCG detects Incipient Arrhythmia uniquely and unconventionally, thus it can detect when the conventional EKG fails to detect.
Ventricular Arrhythmia: (Initial early stage)
Ventricular arrhythmias are abnormal heartbeats in the inner area caused by the lower heart chambers, called ventricles. They cause the heart to beat too fast, which prevents oxygen-rich blood from circulating to the brain and body and may result in cardiac arrest.
Myocardial Damage
When an area of the heart muscle (myocardium) is damaged or dies after the blood supply is blocked, it's the classic medical term for a heart attack.
Other causes of myocardial cellular senescence due to loss of mitochondrial energy production functions are metabolic and poorly treated hypertensive heart disease, environmental toxins, pesticides, heavy metals, or harmful drugs, poorly pulmonary or Rheumatic heart disease, surgical instrument injury, blunt chest trauma, in addition to environmental toxins or dangerous drugs, for example.
Myocardial Damage, colloquially known as a "heart attack," is a portion of the myocardium that stops functioning. Myocardial damage may be “silent” and go undetected, or if the extent of the Damage reaches a stage where the loss of functions could be a catastrophic event, leading to hemodynamic deterioration and sudden death.
Myocarditis:
Myocarditis is inflammation of the heart muscle, and pericarditis is inflammation of the outer lining. In both cases, the immune system causes inflammation in response to an infection (e.g., viruses, fungi, bacteria) or some other metabolic heart dysfunctional trigger (e.g., too much Insulin used to treat Diabetes, or hyperinsulinemia due to over-carbohydrate feeding, ultraprocessed food intake) or some other trigger (e.g., acute post-myocardial infarction, chronic cardiomyocyte senescence due to mitochondrial dysfunctions, autoimmune disorders, cytokine storms due to reactions to acute infectious causes, side effects of medications, vaccines, environmental toxins, heavy metal poisoning, pesticides, Alcohol, etc.).
Pulmonary Heart Disease:
Pulmonary heart disease is a rare condition caused by long-term tobacco smoking, COPD, and Asthma in which the heart cannot pump enough blood to the body. It usually begins with pulmonary hypertension, or high blood pressure in the arteries inside the lungs. Pulmonary hypertension is a condition that specifically affects the arteries in the lungs. The causes can be long-term tobacco smoking, COPD, Asthma, and others.
Rheumatic Heart Disease:
Rheumatic heart disease occurs when the heart valves or other structures suffer Damage due to rheumatic fever or other inflammatory/infectious/metabolic dysfunction factors. Heart valve damage may start shortly after an untreated or under-treated streptococcal infection, such as strep throat or scarlet fever. An immune response causes an inflammatory condition in the body, which can result in ongoing valve damage.
Congenital Heart Disease:
Congenital heart disease (CHD) is an issue with the abnormal structure formation of the heart present at birth. For example, one has a hole in your heart wall.
Issues with your blood vessels (too many or too few, blood flowing too slowly, to the wrong place, or in the wrong direction).
Problems with your heart valves that control blood flow.
Other inborn errors of metabolism, congenital or genetic defects such as Hunter’s Syndrome, Marfan syndrome, etc
Ventricular Hypertrophy: Left ventricular hypertrophy thickens the heart’s main pumping chamber (LV) wall. This thickening may result in blood pressure elevation within the heart and sometimes poor pumping action.
Right ventricular hypertrophy (RVH) is an abnormal enlargement or pathologic increase in the right ventricular muscle mass, which occurs as a maladaptive response to chronic pressure overload. RVH most commonly arises from chronic, severe lung disease.
Bilateral ventricular hypertrophy also exists and is measurable using MCG.
PHYSIOPATHOLOGICAL CONDITIONS: (For clinicians’ references and pattern recognition purposes only, not definitive diagnosis)

Myocardial Remodeling
Myocardial remodeling (REM) may be a damaging process characterized by gradual cardiac enlargement, cardiac dysfunction, and typical molecular changes. It is a universal phenomenon caused by many pathological conditions, the most common of which is myocardial infarction.
Athletes may assume they have “physiological remodeling.” However, other factors, which can be pathological,” may contribute to the impact.
Decreased myocardial compliance
The term compliance measures how difficult a heart chamber or the lumen of a blood vessel is to extend when it fills with blood. Physically, compliance (C) defines the volume change (ΔV) divided by the change in pressure (ΔP). Conditions such as long-term exposures to Ischemia or hypertension left unmanaged can lead to decreased compliance and, ultimately, heart failure, reduced ejection fractions,
Left ventricular filling is restricted when left ventricular compliance markedly decreases. When left ventricular compliance markedly decreases, stroke volume and cardiac output decrease, with signs and symptoms of low cardiac output. Pulmonary venous hypertension is associated with an obligatory increase in pulmonary artery pressure.
Increased myocardial compliance
Compliance is the inverse of stiffness and describes how easily the heart expands when blood fills up. As the ventricular filling increases, higher filling pressures develop nonlinearly for a given volume. Conditions such as acute myocardial infarction or myocarditis may lead to increased myocardial compliance. Please exercise Caution; caregivers must avoid risky actions such as sending patients to extraneous activities, including stress testing. Increased peripheral systemic resistance can lead to myocardial rupture and sudden death due to increased myocardial compliance.
Decreased ejection fraction
A clinically normal ejection fraction is between 55 and 70 percent. An EF from 41 to 49 hearts might be considered too low. It is important to note, however, that you can have an expected average ejection fraction measurement and still have heart failure. The condition is called HFpEF or heart failure with a preserved ejection fraction. MCG dynamically detects abnormal ejection fractions below 55 percent and then integrates the information into the overall severity scores functionally, physiologically, and mathematically. For nearly 50 percent of patients with clinical manifestations of heart failure, MCG is the ONLY test that can identify these patients, bar none.
Bradycardia:
Bradycardia is a slower-than-normal heart rate. A typical average adult resting heart rate is between 60 and 100 beats per minute (bpm). If you have bradycardia, your heart beats fewer than 60 times a minute. Bradycardia (heart rate 40 – 60 bpm) is typical when sleeping. However, medications, such as beta-blockers and other abnormal autonomic dysfunctions, can lead to abnormally low heart rates than usual.
Tachycardia
Tachycardia means your heart beats faster than expected, usually more than 100 beats per minute. Some forms of tachycardia are typically “normal” in contrast; others can indicate a disease process or be life-threatening, mainly when they occur in conjunction with myocardial compliance issues, V-fib, synchronization, etc.
Acute Power Failure: MCG directly measures power output due to overall mitochondrial energy production dynamics. However, chronic conditions can also lead to persistent power failure, which may be harder to treat. Acute heart failure: Acute Power Failure is mainly due to mitochondrial failure or drastically reduced mitochondrial functions in energy production. Causes can be acute Ischemia, MI, metabolic dysfunctions, neurohormonal disorders, and acute stress. These are potentially reversible. However, Chronic conditions can also lead to persistent power failure, which may be harder to treat and reverse.
Global asynchrony (II < V5):
Global asynchrony in the heart is a delayed contraction of the right side of the heart. It can occur involving the right ventricle (RV) after a myocardial infarction (MI) due to a loss of contractility in the damaged heart muscle or hypertrophy due to hypertensive heart disease. This abnormal function can lead to LV global remodeling and dysfunction. Asynchrony can also relate to regional variation in the timing of diastolic events.
Global asynchrony (V5 < II). Global asynchrony in the heart is a delayed contraction of the left side of the heart. It can occur in the left ventricle (LV) after a myocardial infarction (MI) due to a loss of contractility in the infarcted myocardium. This dysfunction can lead to LV global remodeling and dysfunction. Asynchrony can also lead to regional variation in the timing of diastolic events.
Localized Asynchrony
Mechanical cardiac asynchrony is a delayed contraction of specific myocardial regional segments; one part is out of the “phase” with its counterpart.
Local asynchrony (II < V5): Local asynchrony is a delayed contraction of the right-sided heart segment(s). It can occur in the left ventricle (LV) after a myocardial infarction (MI) due to a loss of contractility in the infarcted myocardium. This dysfunction can lead to LV local remodeling and dysfunction. Asynchrony can also lead to regional variation in the timing of diastolic events.
Local asynchrony (V5 < II): Local asynchrony in the heart is a delayed contraction of the left-sided heart segment(s). It can occur in the left ventricle (LV) after a myocardial infarction (MI) due to a loss of contractility in the infarcted myocardium. This dysfunction can lead to LV local remodeling and dysfunction. Asynchrony can also lead to regional variation in the timing of diastolic events.
My Comments:
The report will sound intimidating to you. MCG has learned these terms from years of data mining and deep learning from the legacy cardiology world. I decided to adopt these terms so we can communicate with the clinicians. Otherwise, those with the best and most brilliant minds will not easily understand and master the mathematical descriptions and digital output. The descriptions of each term are scary to many by design of legacy cardiology. However, please do not fall for it. They are designed to make you feel things are dire, but they are NOT. The good news is that there are simple things you can do for yourself to improve your mitochondrial functions and, thus, your metabolic health, and make more of them to reverse these trends. We have proven that.
Here they are:
Maintain a daily happy and positive attitude towards life, no matter how challenging and stressful. Be a happy warrior, and be resilient. Secure a solid six-hour uninterrupted sleep in total darkness.
To reach maximum heart rates, exercise regularly, practice high-intensity interval and weight training to build muscles, and do short bursts of rapid running three times a week to maintain maximum heart rate for a brief burst of time (~90-120 seconds).
Eat whole foods and avoid ultra-processed foods (seed oils, sugar, flour, and chemicals you do not recognize reading the ingredient lists). Learn the art of intermittent fasting and fasting to improve your mitochondrial functions and autophagy, and practice high-intensity interval training and short bursts of anaerobic exercises to grow your muscle strength and mass.
These will go a long way toward improving your metabolic health and adding new, fresh mitochondria to your cells. MCG can measure the improvements following these simple lifestyle optimization measures without adding more drugs to your burdened life.
There are plenty of examples where you can learn how lifestyle optimization can help you reverse and eliminate these scary terms in your following MCG report! We have witnessed these startling life-changing moments in patients treated “maximally” with PTCA/Stenting, Coronary Bypass Surgeries, and on multiple medications that benefit from these lifestyle measures. Initially, they were shocked to learn from their MCG reports that their “maximum treatments” were not enough, and then, they were relieved to discover that following these simple measures, the conditions improved measurably.
Most importantly, MCG’s early detection capabilities will help you detect the earliest signs of mitochondrial dysfunction due to metabolic problems, allowing you to reverse these trends, prevent the progression of chronic diseases, stay healthier, and live longer without too much medical intervention for the overwhelming majority!
Help has arrived!
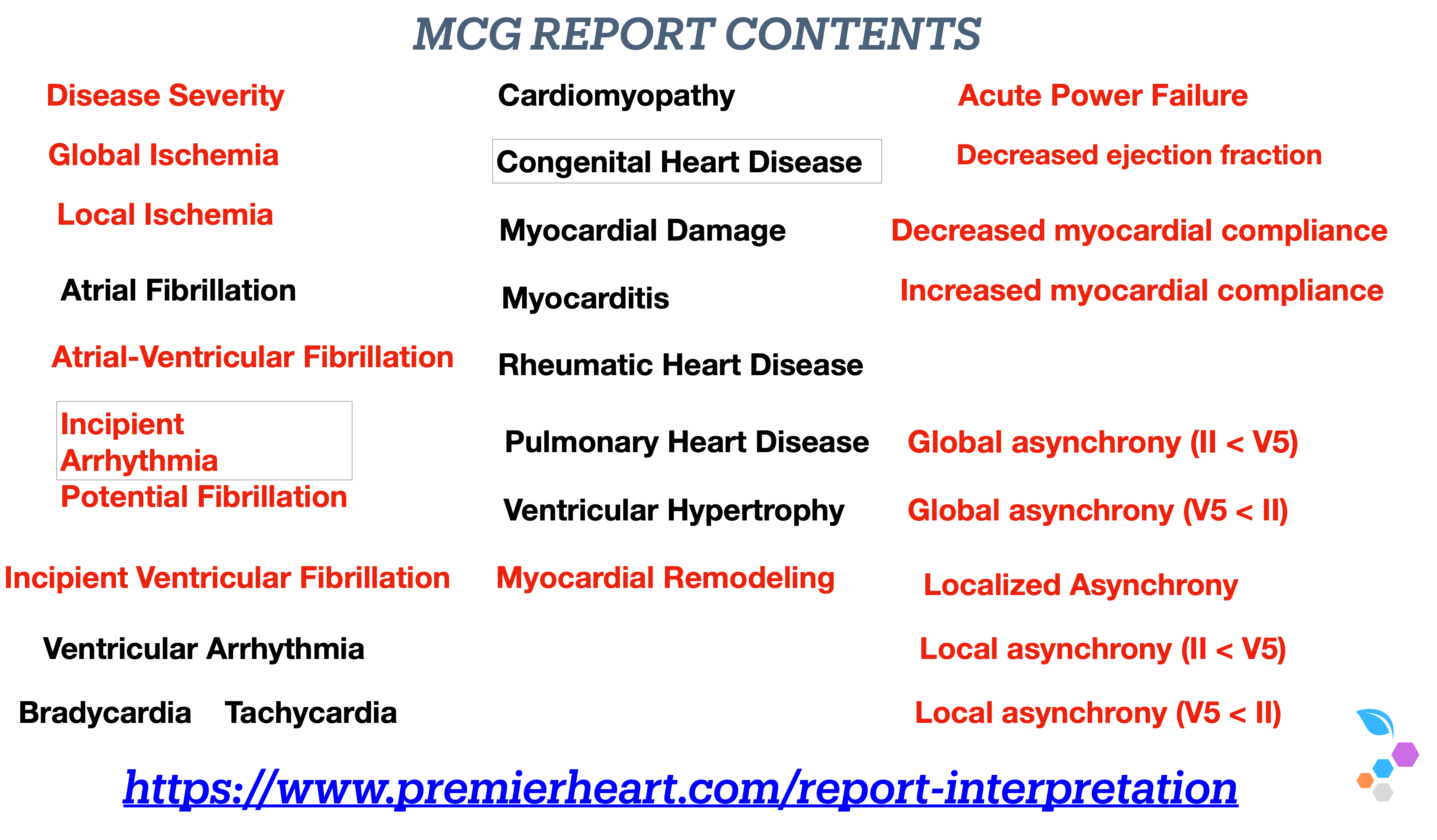
In summary, our two generations of dedicated work have filled the gaps in the allopathic diagnostic arsenal’s blind spots in Eighteen (18) RED, which we have discovered and thoroughly validated to maximize MCG‘s safety and effectiveness, and Eleven (11) BLACK, which is known to the traditional allopathic world and indicates a limited perspective of the conventional. These Twenty-Eight (28) Features provide information that otherwise would be unavailable anywhere else, helping clinicians make bedside diagnoses faster, more accurately, cost-effectively, and safely.
Physicians have blind spots in understanding the system’s physiological responses to complex diseases.
Premier Heart’s MCG Technology is a domain-intelligent systems physiological tool designed to solve complex problems, fill physicians’ knowledge gaps, and assist them in making better diagnosis and treatment decisions.
Managing chronic diseases is complex.
Physicians have blind spots in understanding the overall system’s physiological responses to complex diseases.
MCG is a domain-independent deep machine and human learning neural network computational systems physiological tool designed to solve complex problems. It aids physicians in making better diagnoses and treatment decisions.
MCG is also a model of how companies building AI in medicine should follow:
Rule and first mathematical principles driven, built upon 💯% empirical data without the failed “expert opinions and scientific consensus” based, often plagued with corruption and captured profit-motivated propaganda to sell pharmaceutical products, surgical procedures, and devices in the allopathic medicine world.
We have insisted on conducting honest, objective, and highest-quality verification and validation to ensure effectiveness and maximum safety for the patients.
Convenient, practical, reliable, cost-effective, and most importantly, accurate and quantitative information and analysis to save lives, prolong health span, at affordable costs.
Premier Heart’s MCG is saving and prolonging countless people’s lives, as we are witnessing.
Below are some real-life examples:
For further questions, please get in touch with info@PremierHeart.com.
Our reality-based DML/NN system, built on shoestring budgets over the years, is anchored on a set of immutable and immortal mathematical principles reflecting the physiology of human biology supported with solid, vetted, reliable, trusted, and objective training data sets devoid of the unscalable backward legacy analog medicine’s biased “paid-expert-opinions-based” and against amoral dehumanizing “profit-only-motivated” agenda. We have repeatedly optimized the MCG tech platform reporting accuracy to save lives for the lowest costs. This 21st-century scalable forward-looking digital “100%-empirical-evidence-based” diagnostic information digital technology solution has taken us two and a half generations and decades to create; we have reliably solved critical medical diagnosis issues to support patient-centered decision-making to restore the lost trust and confidence in the failed 19th-century legacy “only-trusting-the-experts” medicine; in addition, we also have the monetization models figured out already.
Here are some examples of how we help people with “invisible” metabolic dysfunctions impacting their hearts:
And our journey to validate our claims in real-world clinical settings through blinded independent cream-of-the-crop ethical volunteering investigators without any industry standard, but corrupt quid pro quo:
The Journey to Freedom of an emancipated enslaved physician

Edited and updated version of the Chapter 12 Multifunction Cardiogram, a.k.a. MCG Technology, Mark Houston’s “Personalized and Precision Integrative Cardiovascular Medicine” 1st Edition Joseph Shen, MD, Raffi Bianchi Shen (Editor),
Enjoy!
Humbly Yours, Joseph
As Arthur C. Clarke once said: "The only way to truly understand the limits of the possible is to push past them and explore the impossible." This philosophy guides our work at MCG, where we constantly push the boundaries of what is achievable in bioengineering and technology.
Joseph T. Shen, an independent, self-emancipated, recovered, freedom MD, became a self-taught BioCybernetic Systems Information Technology Engineer pioneer focused on developing Computational BioCybernetics and Lagrangian Mechanics Systems Engineering Deep-learning heart and brain-saving Intelligent Technologies.
Researcher and Technology Developer
Managing Member
Premier Heart, LLC
Premier Heart International, LLC
Premier Heart Japan, Inc.
Emergency MCG USA, Inc.
110 Main Street, Suite 201-88
Port Washington, NY 11050
Tel: 516-883-3383 ex 8102
Fax: 516-883-5812
Mobile: 516-603-6368 (Please alert me who you are with a text message first; please do not respond to unknown numbers. I WILL respond as soon as possible.)
Email: jtshenmd@premierheart.com (mailto:jtshenmd@premierheart.com)
https://open.substack.com/pub/mcgdoc/p/we-have-built-the-worlds-first-reality?utm_campaign=post&utm_medium=web