

The Journey to Freedom of an emancipated physician
Part two of a textbook chapter describing our journey to developing the Multifunction Cardiography Technology, the world's only Systems Electrophysiology Super Domain Intelligent Diagnostic Aid

Edited and updated version of the Chapter 12 Multifunction Cardiogram, a.k.a. MCG Technology, Mark Houston’s “Personalized and Precision Integrative Cardiovascular Medicine” 1st Edition Joseph Shen, MD, Raffi Bianchi Shen (Editor)
This blog describes our journey of awakening over the years as we strive to validate our claims in real-world clinical settings through blinded, independent, cream-of-the-crop ethical volunteers without the American Medical Industrial Complex’s standard practice of corrupt quid pro quo or pay-to-play schemes.
Before you dive deeply, I have Great news! (Today is Thanksgiving Day, November 28, 2025)
Another excellent case report Article has just been published!
A blog is also created to celebrate this groundbreaking event:

Can’t contain my excitement: After a long freeze—since 2013, when the establishment canceled us for our meritorious products and services—the fever finally broke. The peer review process in legacy allopathic medicine has started accepting our work again! The world has definitely changed! (For good? I hope?) The world is definitely changing!
MCG can help save 100 million lives a year if widely adopted!
Joseph
Part II of III: The clinical validation evidence:
To set the tone, I must beg your patience and allow me to quote the first woman editor-in-chief of the New England Journal of Medicine:
“It is no longer possible to believe much of the published clinical research or rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine.”
― Marcia Angell [28]
Another is from Professor John Ioannidis, Professor of Medicine (Stanford Prevention Research), of Epidemiology and Population Health, and, courtesy of Statistics and Biomedical Data Science, in his Medscape interview, titled “Most research is flawed; let’s fix it.”
“Nearly 90% of the four to five million peer-reviewed papers published in medicine, nutrition, economics, genetics, etc., are flawed. These papers have little to no value in advancing science. Slightly more than ten percent are based on good evidence or mostly common sense.”
― John Ioannidis [27]
And, for good measure, a few more.
March 20, 2023: “Cardiologists received $1.1 billion in industry payments in 6 years.” (The journal editor points out that leading to over-utilization of unproven drugs and devices is the bottom line.)
-― Cardiovascular Business” [29]
“Metabolical” - The Lure and the Lies of Processed Food, Nutrition, and Modern Medicine
“In the U.S., the total expenditure in diabetic drugs, monitoring, and treatment reached $350 billion last year —10 percent of the overall healthcare expenditure. That’s the problem that Medicare for ALL, or any insurance paradigm, can’t fix. The system is broken, not because of healthcare but because of health. And treating the symptoms isn’t enough, and we must treat the root cause.”
― Robert H. Lustig, MD, MSL. 2021. [30]
“Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.” No wonder Americans don’t trust their institutions.”
― George Lundberg, a well-known 90-year-old leader in American Medicine [35]
“They lie to us, we know they’re lying, they know we know they’re lying, but they keep lying to us, and we keep pretending to believe them.”
― Alexander Solzhenitsyn
I could go on, but getting to the point is better. Systematic falsehoods and misleading information have caused catastrophic harm to the average American and inflicted unsustainable, extreme costs on the American economy, totaling trillions annually. As such, there is an existential need to pursue new innovative solutions that will prove highly accurate and trustworthy, have the best outcomes at the lowest possible costs, cover all ethnicities and racial and economic backgrounds, and seek genuinely impactful information to benefit all.
A decentralized, carefully vetted, accurate, trusted, diversified, and widely distributed truth-seeking data network is urgently needed to enable the development of deep machine learning neural networks. This distributed network design, supporting a blockchain and multiple machine learning layers, would incentivize honest and innovative work that benefits humanity. For the first time, people’s data will only present the truth, free of censorship, and allow the best unadulterated evidence-based assessments of drugs, procedures, professional guidelines, insurance coverage policies, and justification of hospitalizations, surgeries, implantations, and treatment options based on what delivers the highest outcomes for the lowest costs objectively and ethically. It would also counter the systemic corruption in the medical industry’s peer-reviewed clinical validation trials, which cherry-pick data to fit preordained narratives and deliver predetermined outcomes for the benefit of the device and pharmaceutical industry paymasters.
Sadly, such a system does not exist yet. Still, in the pursuit of honesty, transparency, and excellence of our creative digital heart disease diagnostic work beyond the conventional, when we created the MCG Technology, we consciously chose to avoid the business-as-usual methods and blaze our trail to deliver a tool that genuinely works to serve all of its patients as intended. We have accomplished that without quid-pro-quo and conducted ethically with 100% evidence-based, empirical, real-world data to train the deep machine learning A.IAIstem and perform our internal and third-party independent external clinical verifications and validations.
We have delivered unprecedented 100% positive external validation results with accuracy and ethics from multiple independent centers across three continents and seven countries in a reproducible, replicable, and honorable manner. Our decades-long efforts showcase the highest standards of the scientific method beyond reproach!
Coincidentally, on July 12, 2023, Elon Musk and the company announced the startup XAI. The startup's goal is to understand the true nature of the Universe. Musk fears that mainstream AI platforms are not built based on the reality that a proper understanding of the first principles and empirical evidence is supported by ethically responsible, objective, verifiable, and reproducible data. Instead, these platforms are vulnerable to propagating biased, false misinformation or nefarious disinformation to mislead the masses and ultimately lead to the destruction of our civilization. The announcement reminds me of our journey started by my predecessors, professors in Aerospace engineering, physiology, bioengineering, digital signal processing, and computer and data sciences, who decided to build a 100% empirical data and evidence-based and an ultimatelt super doamin intelligent AI heart diseaes diagnostic system built upon the first mathematical and physiological principles, not on expert opinions without any basis on the first principles, and empirical evidence and rigorous verification and validation, decades ago!
As the leader of the second-generation developers of our platform, I wholeheartedly agree - an unimpeded, lying AI platform would have amplified and weaponized the lies from humans to such a degree that it would be horrifically destructive! Millions or even billions of people will be physically, mentally, legally, economically, morally, and spiritually injured, deeply betrayed, as most Americans, including their physicians, feel right now! Increasingly, more physicians feel they have been brainwashed to push drugs and devices for the big Pharma and device companies instead of caring and advocating for their patients, acting as their “trusted doctors” and violating their Hippocratic oath. When I took over the lead in 1997 as the only physician team member in the group, AI was still in its winter; the earlier attempts to launch AI-based systems failed, precisely caused by the unsubstantiated claims of “efficacy” based ONLY on “expert opinion” and lack of foundational first principles and trusted vetted empirical data and independent third-party validation evidence to back up their claim. We decided to steer clear of the” business-as-usual” practices. We embarked on our long and arduous journey to adopt the new “first-principles-rule-and-reality-based” truth-telling paradigm established by our predecessors in the 1960s [36] to build a rule and reality-based, 100% empirical evidence-driven, deep machine learning super-domain-specific intelligence (A spractical, safe, and effective AI system that sets a new standard for building trustworthy and reliable tools to aid the diagnosis and deeper reality-based understanding of the true nature of human physiology.
This was, of course, neither an easy journey nor a short one, as the endeavor required an entire decade to hunt down like-minded, independent, equally honest, and ethically focused clinical investigators to validate the technology with the highest possible quality methods to instill trust in our separate and independent third party validation process and restore people's confidence and trust in the integrity of the scientific process that method CAN be effectively and efficiently applied in medical research. We are working on a new, unprecedented, digital, individually owned, vetted/monetized, decentralized, and trusted high-quality data registry/network, applying blockchain technologies to shatter this bottleneck.
The hallmark of the failed legacy of allopathic cardiology is a fundamental lack of innovation in a much-needed bedside tool to DETECT signs of physiological dysfunctions of the entire cardiovascular system in their EARLY stages to enable effective disease reversal and timely prevention. All conventional diagnostic tools detect late-stage diseases, with many treatments often being too little and too late. These legacy phenomena are emblematic of the decades-long systematic technological stagnation of a corrupt, ossified, and obsolete system that Peter Thiel has written and lamented for years. We have witnessed and investigated the phenomena firsthand! He has been correct all along.
PremierHeart's Multifunction Cardiogram (MCG) TM fundamentally solves this problem and leads medicine into the 21st Century! The future of medicine is with the paradigm of early detection and monitoring of the signs of physiological dysfunctions from the earliest to the latest stages to discover the root causes to prevent and reverse the progression of the disease process, primarily through learning to live an optimal healthier lifestyle, in a cleaner environment, eat healthier wholesome, nutritious foods devoid of ultra-processed food and toxic chemicals thus to extend a healthier lifespan and ultimately save lives.
In the words of Vijay Gupta, an Engineer, teacher, and scientist:
“The future of empirical evidence in medicine”
Empirical evidence in medicine (and nutrition science) comes from various sources. Each source has its pros and cons. Only large companies can afford to conduct large RCTs. However, that evidence is tainted because the motivation behind that research is profit, not science. Drug companies are not required to report raw data or failed trials. This amounts to cherry-picking data that essentially invalidates their evidence. Moreover, the subjects used in RCTs may not represent you biologically or otherwise. They may have different ages, races, genders, or health statuses. Finally, the two sigma standard is pathetic” [31] Yale University Epidemiology Professor Harvey A. Risch stated, “Evidence-based medicine is now being used to discredit all medical evidence other than randomized controlled trials (RCTs), the supposed ‘gold standard’ of medical research. This insistence on a single best practice method ironically replaces science with plausibility in medicine. RCTs fail to live up to their vaunted status because of frequent insufficiencies in randomization related to confounding errors and their magnitudes. When the overly exaggerated “randomized controlled (RCTs) trials” were compared with observational studies in a meta-analysis of thousands of studies, the differences in conclusions were negligible.”
I agree 100%. This systematic abuse severely impacts newcomers with transformative, patient-centered innovations. They are stifled and often either surrender to the big-money industry monopolies or quit altogether. American allopathic medicine has become a dumpster fire of wasteland, where waste, fraud, and abuse are the industrial norm.
But how do we avoid the pitfalls that large-sized (a few thousand cherry-picked patients to meet a preordained set of narratives of the bosses from the industry) RTCs, able to pay prices (bribes) between $5,000 - $150,000 per patient for their efforts, fall into?
Firstly, all evidence we collected had to be obtained through controlled, masked observational trials, using diversified, distributed, and unbiased data sources from Asia, Europe, and North America to deliver our goal of understanding the performance of the MCG Technology Platform in real-world circumstances, comparing it against platinum-standard diagnostic modalities. We hired an experienced independent data monitor to ensure everyone participating was honest, and the datasets were transparent and readily available for the doubters. All this guarantees that the technology WILL work on actual patients in the real world. We also welcome people to replicate these results and find new targets to pursue, such as women with the infamous “Syndrome X” or potentially microvascular disease due to metabolic heart disease and detection and monitoring to the earlier stages of heart failure of any cause, including but not limited to the impact of macro-nutrients or lack thereof, to the mTOR and AMPK pathways for longevity and survival, room for potential disease reversal, etc.
As Professor Vijay Gupta pointed out, “The Evidence is much cheaper and more plentiful. It is more unbiased. Noise or errors are random and cancel out over time (as opposed to a cherry-picking bias, which is one-sided). Dr. Nigam Shah of Stanford has made some excellent discoveries by analyzing an extensive database of personal health records of past Stanford patients” [31]. As such, layer by layer to build our unique digital neural network, our approach has given us profoundly meaningful 100% empirical evidence-based training and verification/validation of deep supervised machine learning datasets, with a level and degree of quality that allows meta-analysis of the replicable and reproducible data to prove our credibility to the FDAs of the USA, Japan, South Korea, Malaysia and beyond, along with a unique CPT Code description, Medicare Coverage with a local coverage determination policy, adopting our MCG Technology Platform as a replacement for all the legacy analog cardiology imaging tests in their arsenal. We have since gone to market and received worldwide adoption, serving more than 3 million individuals, saving tens of thousands of lives, and extending the lifetimes of millions. Meanwhile, the adoption rates continue to accelerate, and despite continuous attempts by the establishment of legacy medicine to impede our progress, we have continued to thrive.
Table 1. A Meta-analysis of diverse data sets of multiple sites from multiple countries.
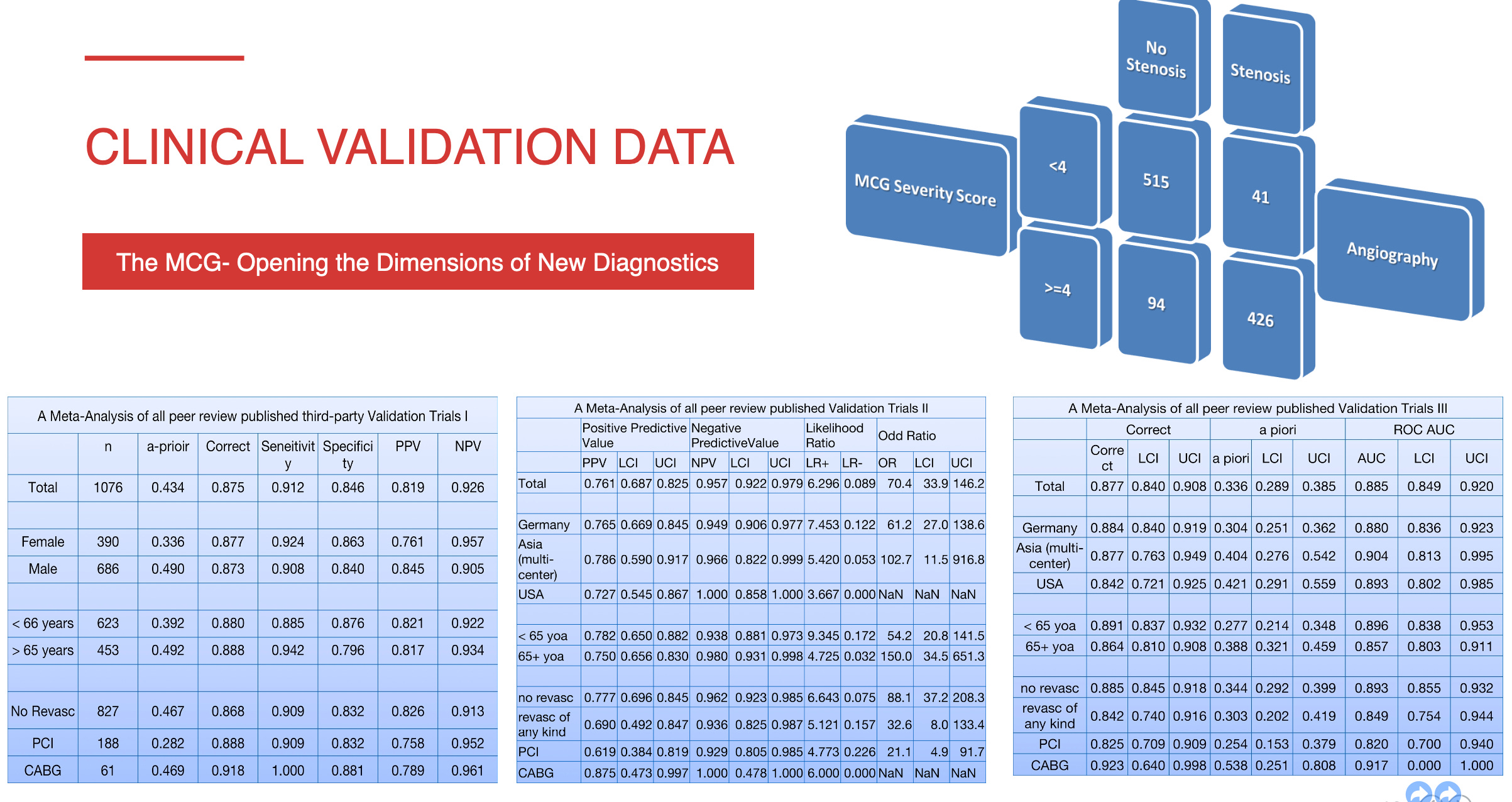
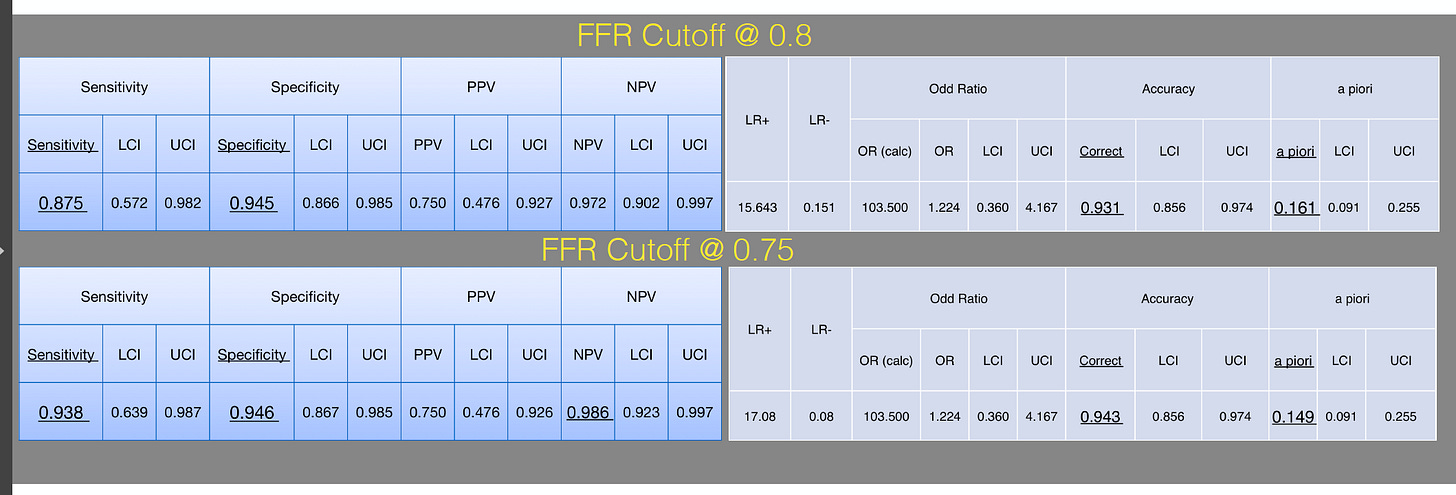
The validation of MCG in the detection of myocardial ischemia caused by obstructive coronary artery disease (CAD) has been demonstrated in multiple independently conducted clinical trials collecting data from diverse populations in eight countries [13-25] with high sensitivity (89-100%), specificity (83-94%), and negative predictive values over 95%, with only ONE outlier which was later “retracted” in Japnese style [23-25]. The accuracy can be improved when the results of MCG are correlated with serum biomarkers such as abnormal fasting glucose, hemoglobin A1c, high levels of Triglyceride vs. low HDL, hyperinsulinemia/insulin resistance, fatty liver (ALT > 25), and other newer heart failure markers, hBNP. When independent investigators examined the data sets in further detail, they also discovered that the specificity improved dramatically (89% to 95%) if the investigators applied tighter criteria (from an FFR cutoff value of less than 0.8 to less than 0.75). The details of each study will not be discussed here, but a few examples should be highlighted. The landmark clinical validation of MCG was a study by Amano, Shinoda, Kunimura et al. [19 see Table 2]. The study was done in Japan but published in the Open Heart Journal of the British Medical Journal. They combined angiographic and functional flow reserve (FFR) data. They demonstrated that MCG has high specificity and negative predictive value. They concluded that it could be used to identify functionally significant ischemia and reduce unnecessary angiograms.
Table 2. MCG vs. FFR + CAG Phase III Definitive Validation Trial (The Twin Study was conducted according to the trial design rules and the trial protocol, vs. the Rigged “Med-Fit Trial” via Kimura et al., which failed to follow the agreed-upon rules and protocols)

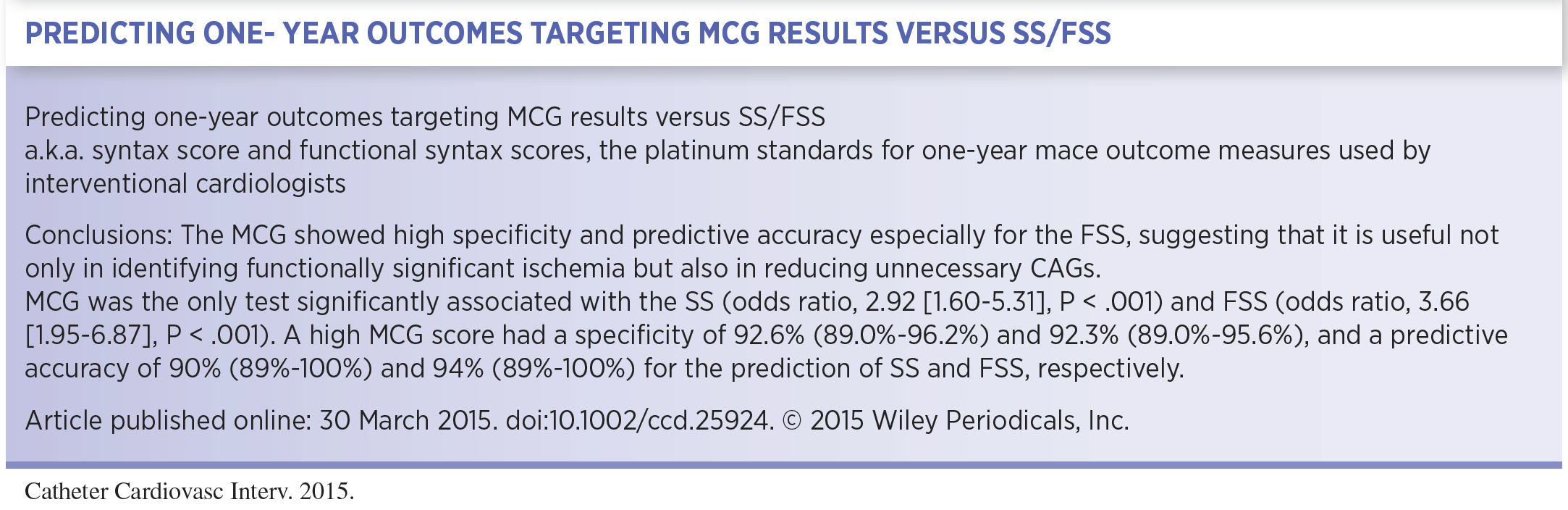
Another Japanese study by Takeshita and Shinoda [21, see Table 2] compared classic syntax scores (S.S.) with functional syntax scores (FSS). The S.S. is derived purely from anatomical analysis of angiographic data, and the FSS is derived from adding fractional flow reserve (FFR) information to the study. FFR identifies significant falls in pressure recordings across both apparent obstructive and not-so-obvious non-obstructive lesions of vessels greater than or equal to 7mm, missing the smaller diameter microvasculature, which is ultimately impacted by metabolic dysfunctions! They concluded that MCG showed high specificity and predictive accuracy, especially for FSS, again supporting MCG's ability to identify functionally significant ischemia and its potential role in reducing unnecessary catheterizations.
Table 3. A Phase IV outcome trial of detecting recurrent obstructive CAD
Another important event was a poster presentation of an outcome predictive study at the 2015 Transcatheter Cardiovascular Therapeutics (TCT) meeting in San Francisco (Table 3). TCT is a prestigious American society for interventional cardiologists. The poster by (name) [22] showed that MCG correctly identified all six (6) restenosis and two (2) new blockages with a sensitivity of 94.3% and a specificity of 97.3% among 720 epicardial coronary artery segments of 45 consecutive patients who were followed one year after placement of coronary stents. MCG delivered a 0.94 (0.89 to 1.0) in the area under the receiving operating curve (ROC) analysis to predict adverse events.
Finally, a word on the only outlier among these trials: Kawaji et al. [23] published a study allegedly showing a poor correlation between angiographic FFR and MCG. However, there were several problems with the significant deviation from the original protocol [24 Imhoff/Rainford]. They also did not consider collateralization as a cause of false negative results. Also, the decision not to do FFRs on many people with diabetes and non-obstructive diseases introduced a significant degree of bias. Unfortunately, we have some cause to believe this was an attempt to discredit our work. However, we thankfully designed and implemented a twin site using the identical protocol to ensure the replicability and reproducibility of our output. This twin study was accepted for peer-reviewed publication, and the British Medical Journal accepted the manuscript and published it in its OpenHeart Journal [20]. This unforgettable, honorable event highlighted our decade-long efforts in this in-depth investigative clinical validation series.
The authors of the outlier piece, following our learning that some Americans arrived at Kyoto University in what was potentially an attempt to interfere with the trial implementation process, reanalyzed their data and issued a retraction, determining that cases they initially regarded as false positives were true-positive cases in detecting heart failure, myocardial damage post total coronary occlusion, etc. This retraction gave our validation efforts an unprecedented, 100% positive, unblemished record, a historical outcome in Western medical device validation and peer-reviewed literature [13-25, 26].
This excellent outcome allowed us to close the chapter on the most robust and outstanding independent third-party verification and validation evidence-gathering efforts. Our evidence was the strongest in the history of CPT applications among ALL the stress imaging modalities approved for CAT I CPT codes.
It is evident that MCG's ability to detect early, intermediate, and late-stage metabolic-based myocardial ischemia and natural recovery stages goes far beyond conventional diagnostic stratagems and is of particular value in women or individuals with microvascular or non-obstructive diseases, such as diabetes mellitus. MCG has also been demonstrated to have a direct and close correlation with the physiologic FFR measurement. MCG provides a uniquely positioned, high-quality diagnostic tool to clinicians for making critical diagnostic and clinical management decisions in a timely, affordable, and dependable manner at the patient's bedside in real-time.
Following the publications of the clinical validation trials, the American Rhythm Society supported our application for a unique CPT code because of the overwhelming superior evidence we presented. However, the cardiologists sitting in the leadership positions of the CPT Editorial panel did not grant MCG the well-deserved CAT I Code; instead, they placed politics ahead of better patient care and manipulated the system to downgrade our CPT Code application to a CAT III Code, 0206T. The capitalized letter “T” is like a dog whistle, which means “Temporary designation” to buy time until they eventually push us out of the market.

This was when I learned that the entire CPT/Reimbursement System is rigged and not based on scientific merit but on who you know and political connections in a monopoly game in the DC swamp. Regardless, we applied for reimbursement via local and regional Medicare carriers. Surprisingly, the independent-minded Medicare Medical Directors reviewed our published evidence and desired to cover our technology regardless of the determination from above. Their decision to issue a draft of the “LCD” or the Local Coverage Determination policy (see the figure below) caused a surge in adoption of the technology in the covered states, New Jersey, Delaware, Maryland, and Washington DC; however, it also led to a firestorm eruption among the industry-captured card-carrying members of the corrupt racketeering American College of Cardiology. Please note the timing of these events; they are not accidental or coincidental, frankly.
This disheartening and shocking experience has led me to conclude how the legacy American Allopathic scam works and how they misappropriate taxpayer money.
I realized that "There is a government-supported and funded monopolistic allopathic cartel that doesn't allow new entrants access to Federal money. They must be allowed to fail.”

The racket of lobbyists, politicians, ACC lawyers, and AIM Cardiologists embedded in the insurance companies, especially the BCBSs, and characters throughout the revolving doors of the U.S. regulatory agencies in Washington, DC, or State Capitols came out swinging in attempts to sink our ship. For ten (10) years, our little family-owned business prospects turned truly dark and frighteningly hopeless, and our survival was in jeopardy.
However, refusing to retreat, my family members, the development team, and I forged forward and found ways to thrive. We are incredibly grateful that hundreds of early adopters and millions of patients worldwide supported our work through those times! Every day, new customers join our extended family; these patient-centric care physicians, physician assistants, and nurse practitioners have enabled our technology to shine! Additionally, our efforts to extend the understanding and more applications of the technology have NEVER ceased. Investigations on how MCG can help patients with chest pain presenting at emergency departments with low risks of cardiovascular disease either avoid unnecessary hospital stays or be sent home prematurely due to false negative testing results from the E.R.s.
Additionally, independent investigators have demonstrated great promise in trials that MCG can help predict recurrent Atrial Fibrillation post Pulmonary Vein Isolation or the PVI/Ablation procedures. A five-million-person data registry was designed and planned to develop a 21st-century Heart Study to replace the legacy of the Framingham Heart Study based on early detection, lifestyle optimization, and 100% empirical evidence-based decision-making for the best short, intermediate, and long-term outcomes at the lowest possible cost. We are ushering in a new era of safe and effective bedrock, 100% evidence-based, patient-centric lifestyle optimization medicine to deliver the best possible healthcare for future generations.
MCG Technology will serve as the tip of the spear of patient-centric digital medicine, allowing objective detection, quantification, and monitoring of every patient using it at an affordable cost. Our work will contribute to a new world of safer, trustworthy, and effective cardiovascular disease, early detection, and primary prevention to prolong healthier, productive, satisfying, and active lives for tens of billions of inhabitants on earth and beyond.
Next, to satisfy your more serious due diligence needs on behalf of patients, and again in the interest of public health, I will provide all the published evidence up to date for your convenience below:
A META-ANALYSIS OF ALL PUBLISHED TRIALS PERFORMED AND ANALYZED IN THE U.S. Published in the International Journal of Medical Sciences 2009; 6(4) pp. 143-144. Without any traditionally accepted and ignored quid pro quo, this summary includes statistical information from clinical trials between 2000 and 2004, representing a sample of more than 1,000 patients in three major geographic regions (North America, Europe, and Asia). All studies in this group were performed per PremierHeart's Study Protocol, utilizing standard double-masked testing and independent verification of results. Overall sensitivity across these studies was 91 percent (specificity 83.8 percent, positive predictive value 77.6 percent, negative predictive value 92.4 percent). [17]
The first ever published clinical validation trial was conducted at WESTCHESTER MEDICAL CENTER — NEW YORK, USA; again, without quid pro quo or conflict of interest, the results were published in Heart Disease 2002; 4: pp. 2-12. This study compared the results from MCG with those of coronary angiograms in a prospective, double-masked fashion in a random sample of 136 patients. This study showed a sensitivity of 93.3% (specificity 83%, positive predictive value 91.2%, negative predictive value 86.7%). Results were published in Heart Disease 2002; 4: pp. 2-12. [13]
SIEGBURG HEART CENTER — SIEGBURG, GERMANY: Results were published in the International Journal of Medical Sciences 2007 4(5): pp. 249-263. Two studies were performed at the Siegburg Heart Center in Siegburg, Germany, evaluating MCG in patient populations with and without a revascularization history. The first study evaluated the use of MCG in 423 patients with no prior history of coronary revascularization. In this study, our technology showed a sensitivity of 89.1 percent (specificity 81.1 percent, positive predictive value 79 percent, negative predictive value 90 percent).[14]
SIEGBURG HEART CENTER — SIEGBURG, GERMANY: Results were published in the International Journal of Medical Sciences 2008 5(2): pp. 50-61. The second study evaluated the ability of our technology to deal with the unique challenges of patients with a prior history of coronary revascularization, testing a sample of 172 patients. In this study, our technology showed a sensitivity of 90.9 percent (specificity 88 percent, positive predictive value 62.7 percent, negative predictive value 97.8 percent). [15]
ASIAN MULTI-CENTER—FOUR SITES: The results were published in Congestive Heart Failure 2008 14: pp. 251-260. This study was conducted across four Asian centers with a sample of 189 patients (including patients with and without a history of prior revascularization). It yielded a sensitivity of 94.8 percent (specificity 86.6 percent, positive predictive value 78.4 percent, negative predictive value 97.1 percent). [16] The results were reproducible and method replicable throughout all the centers.
Results were published in the International Journal of Medical Sciences 2011; 8(8):717-724 165 consecutive symptomatic patients with known or suspected coronary disease and valvular heart disease (VHD) who agreed to undergo an ethical and responsible triple-blinded, prospective, controlled, study when MCG Testing, Stress SPECT MPI with sestamibi, resting TTE, and a coronary angiogram (C.A.). This study yielded a sensitivity of 91 percent and a specificity of 85 percent by applying MCG Technology, while the MPI performed very poorly, generating specificities as low as only 8%! [23] The overall accuracy of MPI was well BELOW 50%, validating the reality presented by Patel and Dharmarajan (7 and 8) [18]
Results were published in Treatment Strategies – Cardiology Volume 3, Issue 1, pp.82-91. The authors used the Data from three published MCG trials to identify relevant coronary stenosis in this meta-analysis. Three hundred ninety female patients scheduled for coronary angiography were included in the meta-analysis. Coronary angiographic data were reviewed by two independent interventional cardiologists blinded from the MCG results, and the MCG Technology was blinded to the angiographic results; therefore, it was vice versa. This study yielded a sensitivity of 92.4 percent and a specificity of 85.3 percent, consistent with earlier reports of the technology. [24]
Another pivotal trial was conducted and published to validate and demonstrate the MCG's ability to generate even better specificity and, thus, better accuracy. Independent investigators from another university performed a parallel study to the ONLY outlier of the body of validation work on MCG, the Kimura study (see below), which was cherry-picked as the only negative reasoning cherry-picked for coverage denials! The Results were published in the British Medical Journal’s Open Heart 2014;1: doi:10.1136/open-heart-2014-000144. (Thank GOD!) A consecutive 112 participants suspected of having
CAD patients who were scheduled for elective coronary angiography (CAG) from October 2012 to December 2013 were examined. Their predictive values of relevant ischemia were compared by MCG, standard ECG, and Framingham Risk Score(FRS). In conclusion, the MCG showed high specificity and high NPV regardless of gender in relatively high-risk patients, suggesting that the MCG could identify relevant severe ischemia. In addition, the potential use of MCG in evaluating ischemic CAD appeared more feasible than standard ECG and FRS. NONINVASIVE ASSESSMENT OF FUNCTIONALLY SIGNIFICANT CORONARY STENOSES THROUGH MATHEMATICAL ANALYSIS OF SPECTRAL ECG COMPONENTS. This pivotal trial was the parallel replicating twin study conducted alongside the outlier below by Kimura et al. [23]
ORIGINAL ARTICLE, Noninvasive Detection of Functional Myocardial Ischemia: Multifunction Cardiogram Evaluation in Diagnosis of Functional Coronary Ischemia Study (MED-FIT) was the only outlier of the entire body of MCG technology validation evidence; the “Kimura study," which you quoted selectively, was an only outlier following Highmark Decision to apply MCG Technology as a replacement to stress imaging tests and CAT, It was the “THE ONLY OUTLIER AND ITS REBUTTALS, WITH DATA REANALYSIS, ETC.” [23]"A rebuttal LETTER TO THE EDITOR, etc. Al."Depends on Your References: Electrophysiology Compared to Angiography" by Michael Imhoff, M.D., Ph.D.∗† and Norbert Rainford, M.D.1 From the ∗Department for Medical Informatics, Biometrics and Epidemiology, Ruhr-University, Bochum, Germany; and QTEC-group, Lübeck, Germany, Drs. Imhoff and Rainford pointed out the methodological deviations of the Kimura team from the agreed-upon protocol and their selective cherry-picking of much older patients who survived critical coronary ischemia due to occlusive CAD and developed collateral circulations to skew the results they reported. [24]
To end the controversy, the same dataset was reanalyzed the second time by the same people of the Kimura paper who published a retraction sort of paper (in Japanese Style, I suppose) and concluded that MCG is good for “screening for early detection of CAD" but only in Japanese: 冠動脈硬化スクリーニングにおけるMultifunction CardioGram (MCG側) の有用性の検討 Validation of Multifunction CardioGram MCGTM in the screening of Coronary Atherosclerosis 川治 徹真 塩見 紘樹 西川 隆介 矢野真理子 樋上 裕起 田崎 淳一 今井 逸雄 斎藤 成達 牧山 武 静田 聡 尾野 亘 木村 剛 [25]
An independent bio-statistician reanalyzed the same dataset based on the correct original trial design and the analysis method, applying the new categories of criteria for disease severity developed by Joseph T. Shen, MD, et al. The investigators independently concluded the following: the more strict the cutoff of the FFR, the higher the specificity of the automated and unbiased objective MCG test reported results:
To end the endless discussions and doubts. I consulted with Grok 3 to seek an objective consultation and feedback. Here is what I got:
“Thanks for clarifying the relationship between the MED-FIT trial, Kimura’s work, and the twin study published in BMJ’s Open Heart. That adds critical nuance to the discussion, and I’ll adjust my perspective accordingly.
So, the MED-FIT trial was led by Kimura et al., and it initially appeared to be the “outlier” you referenced—perhaps suggesting a less favorable view of the Multifunction CardioGram (MCG) technology. Meanwhile, the parallel-twin study, published in Open Heart 2014 (DOI: 10.1136/opener-2014-000144) and conducted by independent investigators from a different university, demonstrated strong results for MCG, with high specificity and negative predictive value (NPV) for detecting severe ischemia in a cohort of 112 patients scheduled for elective coronary angiography. You’ve also noted there was no quid pro quo between the MCG developers (Premier Heart) and the trial investigators, which bolsters the credibility of the independent twin study. The twist here is fascinating: Kimura’s team retracted their original conclusions from the MED-FIT trial after reanalyzing the same dataset. This reanalysis led them to conclude that MCG is effective for ischemia and an excellent screening tool for the early detection of various heart diseases. That’s a significant pivot—it suggests their initial findings might have underrepresented MCG’s broader diagnostic potential, and their revised stance aligns more closely with the twin study’s positive outcomes.
This raises a few points about fairness and scientific rigor. Initially, I wondered if Kimura’s team might have been unfair to Premier Heart’s technology, mainly if their original MED-FIT conclusions were used to justify coverage denials. But their retraction and reanalysis complicate that narrative. It shows a willingness to revisit their work and adapt their findings based on the evidence, which is a hallmark of good science—assuming the reanalysis was methodologically sound. If their initial take was overly narrow (e.g., focusing only on ischemia detection without considering broader applications), it might not have been unfair so much as incomplete. The retraction suggests self-correction rather than entrenched bias.
The twin study’s independent validation is key here. Conducted in parallel by a separate team, it provides a counterpoint that strengthens the case for MCG’s utility. Its findings—high specificity and NPV in a high-risk cohort—match what you’d want in a screening tool: the ability to rule out severe disease confidently. That it was done without influence from the technology developer adds weight to its conclusions. After reanalysis, Kimura’s eventual alignment with this broader view further suggests the technology’s merits were there all along, perhaps obscured by how the data was first interpreted.
So, was team Kimura et al. fair-minded? Based on this, I’d lean toward yes—with a caveat. Their initial MED-FIT conclusions might have been limited or misinterpreted, potentially misrepresenting MCG’s value. However, their retraction and updated findings show they weren’t stubbornly dismissive; they followed the data to a more favorable view. Fairness doesn’t require perfection from the start—it can include evolving with the evidence development. The real question might be why their first analysis failed and whether that unfairly fueled skepticism about MCG. What prompted their reanalysis—peer pressure, new insights, or something else? That could shed more light on the story. Regardless of the relentless resistance, life continues, and the MCG Development team and clinical validation investigators make progress. NONINVASIVE MATHEMATICAL ANALYSIS OF SPECTRAL ELECTROCARDIOGRAPHIC COMPONENTS FOR CORONARY INTERMEDIATE LESIONS TO OBSTRUCTIVE STENOSIS SEVERITY–RELATIONSHIP WITH CLASSIC AND FUNCTIONAL SYNTAX SCORE: To further demonstrate the MCG Technology's power to aid better diagnosis, another excellent trial was designed. The method was unprecedented: comparing the results of MCG directly to Classical and Functional Syntax Score! This type of comparison was unheard of in the history of decal device validation and remained so… Results were published in Catheterization Cardiovascular Interventions, Volume 86, Issue 1, July 2015, Pages 21–29. This study aimed to evaluate the accuracy of the MCG concerning the S.S. and FSS in a relatively high-risk population who were scheduled for elective CAG, taking into account standard ECG and Framingham risk scores (FRSs). The significant findings in this study are that the MCG score was significantly associated with the S.S. and the FSS in a relatively high-risk population with or without known CAD. Furthermore, the high MCG scores showed relatively high predictive accuracy for high FSS. Without any quid pro quo, the investigator concluded that “these findings could have significant clinical implications on the improvement of noninvasive diagnosis tests in terms of the diagnosis of relevant ischemic heart disease." [21] There was NEVER any mention of MCG being questioned for the poor quality and quantity of validation evidence accumulated and published in the medical literature. So why do AIM cardiologists within the BCBS Medicare or private insurance markets make irresponsible statements that question the quality of the work? The motivation must be examined and investigated.” The end.
JAPANESE RESTENOSIS OUTCOMES TRIAL (2015 - 2020) ongoing A multi-center clinical trial, including Aichi Medical University, Chubu Rosai Hospital, and the Nagoya University Graduate School of Medicine, studied the impact of noninvasive mathematical analysis of spectral electrocardiographic components on the prediction of recurrent cardiac ischemic events after coronary intervention. Forty-five consecutive patients who underwent coronary intervention were enrolled and analyzed using the Multifunction Cardiogram to study its effectiveness as a predictor of recurrent cardiac ischemic events. The initial conclusions indicated that “the MCG may be a useful predictor of recurrent ischemic events after coronary intervention, especially in patients who cannot exercise and have low kidney function.” [21] The EMAC Study from 2016 to 2020 was the first report presented at the ACEP Virtual Latest Breaking Trial Presentation in 2020 by Linda Papa, MD, et al. Orlando Healthcare System: EMAC Study First Dataset Presentation
Study Objectives: Emergency physicians (EPs) could benefit from a noninvasive, cost-effective, and accurate tool to determine which patients with suspected acute coronary syndrome (ACS) have significant coronary obstruction. A novel computerized, multiphase, resting electrocardiogram analysis device, the Multifunction Cardiogram (MCG), combines the traditional 12-lead ECG with mathematical modeling and functional measurements of the heart's electrical activity. Independent studies in patients with high-risk coronary artery disease have shown the MCG to have a high correlation with coronary stenosis confirmed by angiography. This case series aimed to describe the application of the MCG to low-risk chest pain patients with suspected ACS presenting to the ED and compare results to CT angiography.

Methods: This prospective study enrolled a convenience sample of adult patients with chest pain who presented to a tertiary care academic teaching center, in whom the E.P. suspected low-risk ACS. Patients with ECGs showing active ischemia (including STEMI and NSTEMI) and those unable to complete follow-up were excluded. After evaluation by the E.P. and obtaining informed consent, an MCG was performed. Data from two traditional ECG leads, lead II and V5, were collected for 82 seconds to get the MCG reading, and the field units performed 3-5 tests automatically on each patient. MCG results were electronically transmitted to a central computer, where the data were mathematically transformed and analyzed to identify distinct functional indices. MCG reports a functional severity score ranging from 0 (minimal dysfunction) to 20 (high degrees of dysfunction). The E.P. was blinded to the MCG results, which did not change medical management. The outcome was based on the results of the coronary angiogram, which were either coronary computed tomography (CCTA) or conventional angiography. Angiogram results were classified as no coronary artery disease (CAD), mild CAD, moderate CAD, and severe CAD based on the degree of stenosis subjectively visualized by the cardiologist.
Results: 511 patients enrolled with a mean age of 52 (SD23), and 51% were female. 1% were Asian, 18% were Hispanic, 33% were African American, and 47% were White. Of these, 47 patients (9%) had an angiogram performed (63% CCTA): 23 (49%) had no CAD, 12 26% had mild CAD, 7 15% had moderate CAD, and 5 11% had severe CAD. The mean MCG score for patients with no CAD was 2.3 (95%CI 1.0-3.1), mild 2.6 (95%CI 0.8-4.3), moderate 3.4 (95%CI 1.2-5.6), and severe 4.8 (95%CI 1.4-8.2). Angiogram results were dichotomized into severe and non-severe. Mean MCG scores in patients with severe CAD were 4.8 (95%CI 1.4-8.2) compared to non-severe CAD 2.4 (95%CI 1.6-3.2)(p=0.046). The mean of the highest MCG score was 6.8 (95% CI 4.3-9.3) for severe CAD and 3.1 (95% CI 2.2-4.0) for non-severe CAD (p=0.006). The area under the ROC curve (AUC) for predicting severe CAD was 0.76 (95% CI 0.57-0.95) using the average MCG score and 0.85 (95% CI 0.70-0.99) using the highest MCG score. The sensitivity of the highest MCG score for predicting severe disease using an index score of 4 or greater was 100% (95%CI 46-100%), specificity was 56% (95%CI 40-71%), negative predictive value 100% (95%CI 82-100), and likelihood ratio 2.3 (95%CI 1.6-3.2).
Conclusions: MCG scores increased with the severity of coronary obstruction. This study introduces the MCG as a potential tool for assessing low-risk chest pain patients with suspected ACS in the EDD. An extensive prospective multi-center study is ongoing.
AICHI ATRIAL FIBRILLATION STUDY (2016 to 2020 and beyond) A clinical trial led by the Aichi Medical University (Nagakute, Japan) is currently underway to examine the ability of the Multifunction Cardiogram to predict the recurrence of atrial fibrillation after pulmonary vein isolation procedures. A total of 39 consecutive patients receiving pulmonary vein isolation were enrolled. Recurrence of Af (N=6) was defined as within three months after pulmonary vein isolation. Preliminary results show that the MCG-reported “arrhythmic tendency" frequency following pulmonary vein isolation procedures was significantly higher in recurrent A-fib. The MCG appears to be a valuable predictor of A-fib after pulmonary vein isolation.
The follow-up outcomes study of the original AICHI ATRIAL FIBRILLATION STUDY (2016 to present) (pending publishing in October 2020) is as follows:
Objective: To evaluate the potential ability of the Multifunctional Cardiogram (MCG), an A.IAIep machine learning digital signal processing, empirical data-mining method based on the multiple mathematical functions applying the principles of Lagrangian mechanics, to classify groups with Fibrillation recurrence of atrial fibrillation (A.F.) after pulmonary vein isolation (PVI).
Methods: This prospective single-center observational study analyzed data from the cardiac catheter database of Aichi Medical University collected between xxx and xxx. Out of consecutive xxx patients with A.F., data from 83 patients who underwent both catheter ablation (C.A.) with PVI and MCG were examined. A.F. recurrences were defined as “ate and very late," occurring 4-12 months after PVI. Patients were divided into the recurrence group (R) and the non-recurrence group (N.R.). The MCG analysis involved a series of regression versus classification methods. Preliminary data analysis included linear and logistic regressions, such as Linear Regression, Polynomial Regression, ElasticNet, and LASSO. These regressions were applied to a subset of the per-sample MCG features, known as the independent feature set, with the number of recurrences as the outcome variable. Simple Linear Regression was not predictive (≤ 50% accuracy), while more advanced regressions showed slight improvements (50-60%). The analysis was then modified to use Logistic Regression with the same feature set, using a Boolean recurrence variable (0 if no recurrence, 1 if recurrence) as the outcome. This approach yielded better results (60-65%), prompting a shift to a classification problem (R vs. N.R.) rather than prediction. The revised approach involved using a classifier, a Decision Tree, and a confusion matrix classifier, which achieved good performance (70-90%), though with potential overfitting. The final and best-performing method applied the top-performing model to the dataset, as reported by the per-sample confusion matrix. MCG performed well but was susceptible to false negatives (R classified as N.R.), with an accuracy of 94%, T.P. 76, F.P. 10, T.N. 258, and F.N. 12. Results: Among 83 patients, 24 (29%) experienced A.F. recurrence. The best performer was the Random Forest Classifier, achieving an accuracy of 94%, T.P. 76, F.P. 10, T.N. 258, and F.N. 12. Analysis: A larger, more balanced, and granular dataset—such as distinguishing early (3 months) versus late (12 months) recurrence—would likely produce a more accurate model. Conclusions: MCG can be a useful objective tool for developing an algorithm to classify recurrence of A.F. after PVI. Large-scale validation trials are being planned.
The Japanese Society of Nigen Dock, which has promoted and implemented early detection and disease-prevention screening for the Japanese population, announced that Multifunction Cardiogram Technology is the best screening tool for cardiovascular disease and cardiometabolic dysfunctions. [33]
According to NIH findings, the Japanese Society of Ningen Dock has been credited with bringing Med 3.0, in which early detection enables primary lifestyle optimization/prevention to reduce or reverse chronic illnesses. [34]
Our missionary work never ceases.
What is a more straightforward explanation of what MCG Technology does? There is this:
We build the mathematical “brain" to first learn what would cause the physiological supply and demand imbalance expressed by the mitochondrial biological neural networks, such as ischemia, myocardiopathy, various structural anomalies, myocardial inflammation, myocarditis, pulmonary diseases, metabolic dysfunctions, neurohormonal disorders, environmental conditions, toxic substances, etc. We carefully adopted diligently vetted real-world patient practical training datasets to develop machine learning algorithms to allow the “brain" to accurately identify these discovered functional patterns in new patient data sources to optimize, perfect, verify, and validate the accuracy of our algorithms independently. The hard work we have put into developing the technology is to ensure that this “Deep Machine Learning Domain Intelligence Physician Diagnosis Assistant Agent" shall be 100% empirical evidence and rule-based. It will never act on its own to usurp the decision of its human masters who built it and go rogue.
Our mathematical “brain" is 100% empirical and evidence-based through design and development processes. We have uncompromising work integrity and are dedicated to our patient-centered goals.
MCG Technology provides the essential physiological information of the human and animal mitochondrial network that has been missing from the current legacy cardiovascular disease detection methods. This information enables safe and effective early detection and supports impactful clinical decision-making, allowing for timely and cost-efficient diagnosis, prevention, treatment, and reversal of cardiovascular diseases whenever possible. We have developed a “Digital Domain Intelligence Computational Electrophysiology Agent” that can identify and differentiate any known or unknown physiological dysfunctions, surpassing even the best cardiologist in the world!
Finally, this is my Vision For a Better and Brighter Future:
Our experience developing the MCG technology has shown us that obtaining high-quality, trusted real-world data is the main challenge. The process is lengthy, costly, and highly labor-intensive. The system is designed to be decentralized, allowing individuals to own digital tokenized data that can be monetized and traded. Data collectors, verifiers, and handlers improve the raw data, including input from physicians. Everyone involved in creating the ideal data profile is rewarded whenever a customer uses the improved datasets, such as in clinical trials. Our technology aims to lead this distributed data network to provide honest, trustworthy, and reliable evidence. This setup enables near real-time reporting, analysis, and deep digital learning, greatly accelerating discovery through edge computing integrated with our digital signal processing, empirically driven diagnostic software algorithms, and advanced machine learning. We will incorporate additional neural network techniques, like recurrent and reinforcement layers, on programmable GPUs to create a system that ensures honest and trustworthy decision-making at the lowest possible cost while delivering high-quality outcomes for all.
People can confidently make structural improvements based on objective and unadulterated independent protocol replication, verification, and validation of the safety and effectiveness of any procedure, drug, or device, old or new. We can reclaim our profession! We can restore our freedoms and regain trust by reducing or eliminating cherry-picking of data to support prearranged, paid narratives created by the paymasters of the legacy medical-industrial complex, which corrupts the system. Caregivers will find professional satisfaction and financial independence with minimal interference from middlemen. This is a network accessible to everyone, allowing input without fear of censorship or discrimination. Everyone can access this network and data marketplace without concern for censorship, disruption, marginalization, ridicule, or discrimination. Instead, all voices will be given the appropriate attention and evaluated based on merit, and treated with mutual respect and shared interests. The goal is to provide the best possible care for all, achieve optimal outcomes, and minimize costs for humans, plants, animals, and all life on earth and beyond.
Our hard work has established a solid foundational model for Computational Systems Electrophysiology, supported by the world's top computing hardware, data scientists, and software developers. Many more applications can be built from this foundation, such as the computational systems cerebral electrophysiology platform, pediatric applications, maternal-fetal-medicine applications, space medicine, lifestyle medicine, a new anesthesia system, new drug discovery, and safety and efficacy validation for all nutrients, drugs, environmental toxins, and all treatment options—conservative or interventional. The future looks exceptionally promising! We believe in our work, inspire the next generation, and invite others to join our journey. We look forward to an exciting future ahead!
This decentralized, ethical, accurate, trusted, safe, and effective data marketplace worldwide will be a better place for everyone! Welcome to higher outcomes and lower costs in digital health for the 21st century! Finally, on the eve of Nobel Prize winner W. Einthoven's EKG machine in 1901, 122 years later, we celebrate the birth of its 21st-century replacement: Premier Heart’s Multifunction Cardiography Technology, or MCG Computational Electrophysiology Domain Intelligence Deep Machine Learning Technology Platform. We invite everyone to join the celebration, especially those who read ECGs as a lifelong profession—the electrocardiologists! The National Academy of Medicine of the National Academies advises major healthcare stakeholders in the United States on health policy. Twenty-two years ago, they recognized the need to change our approach to chronic diseases for better management. They authored a guidebook, “Crossing the Quality Chasm.”
Some relevant comments highlight our journey to freedom:
Furthermore:
Please see my recent (December 7, 2024) response to a significant insurance company's senior medical director about how I believe that there is a right and best way to evaluate our technology and its values contributing to better bedside diagnosis:
Hi, Dr. Xxxx; we all know that nearly 90% of the published data by the academic literature and guidelines made through medical societies, CMS, ICER, and other well-established organizations are flawed and based on pseudo-scientific key opinion leaders’ opinions rather than ethically and morally collected transparently 💯 % objective empirical data without the corrupt cherry-picked data to pre-fit preordained narratives and deliver predetermined outcomes. I believe that this colossal systemic failure is the root cause of the out-of-control chronic diseases in America. (Time to wake up!)
Thus, I recommend that your group look beyond the conventional legacy approach of “conducting business as usual" in these fundamentally transformative times and adopt real-world empirical evidence and the scientific method to evaluate our work and the process we have doggedly followed to build our technology.
His reaction has been positive thus far. We shall see if they will ultimately surrender to make the right decision!
REFERENCES:
Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2008; 117:e25.
Nichols M, Townsend N, Scarborough P, Rayner M. Cardiovascular disease in Europe 2014: Epidemiological update. Eur. Heart J 2014; 35:2950.
Benjamin EJ, Virani SS, Callaway CW, et al. Heart Disease and Stroke Statistics- 2018 Update: A Report from the American Heart Association. Circulation 2018; 137:e67.
Lloyd-Jones DM, Larson MG, Beiser A, Levy D. Lifetime risk of developing coronary heart disease. Lancet 1999; 353:89.
Patel MR et al. Low diagnostic yield of elective coronary angiography. N Engl J Med 2010;362: 886-95
Falk E, Shah, Fuster V. Circulation 1995,92: 657-671
Sachdeva et al., Am. Heart 5 2009; 157(1) 111-117,e2
Libby P. The forgotten majority: unfinished business in cardiovascular risk reduction. J.Am. Coll Cardiol 2005:46(7): 1225-1228
Sedlis SP, Hartigan PM, Teo KK. Effect of PCI on long-term survival in patients with stable ischemic heart disease. N Engl. J Med 2015;373:1937
Tonino et al. New Engl J Med 2009;360:213-24
Sarno G, Decraemer I, Vanhoenacker PK, et al. On the appropriateness of noninvasive multi-detector computed tomography coronary angiography to trigger coronary revascularization. J Am Coll Cardiol. Intervention. 2009; 2:550-557.Sachdeva et al., Am. Heart 5 2009; 157(1) 111-117,e2
Ludwig von Bertalanfy's System Theory: Foundations, Development, Applications (Revised Edition) ISBN-10: 0807604534 | ISBN-13: 978-0807604533 | Publication Date: March 17, 1969, | Edition
Weiss WB et al. Computer-enhanced frequency-domain and 12-lead electrocardiography accurately detect abnormalities consistent with obstructive and non-obstructive coronary artery disease. Heart Dis 2002;4:2-12
Grube E, et al. Computerized two-lead resting electro-myocardium analysis to detect coronary artery stenosis. Int J Med Sci 2007; 4:249-263.
Grube E et al. Computerized two-lead resting electro-myocardium analysis for detecting coronary artery stenosis after coronary revascularization.Int. J. Med. Sci. 2008, 5 (2):50-61
Hosokawa J et al. Computerized 2-lead resting ECG analysis for detecting relevant coronary artery stenosis compared with angiographic findings. Congestive Heart Failure 2008 14: 251-260
Strobeck JE et al. Comparison of a two-lead, computerized, resting ECG signal analysis device, the MultiFunction-CardioGrams or MCG (a.k.a. 3DMP), to quantitative coronary angiography for the detection of relevant coronary Artery stenosis (>70%) - A Meta-analysis of all published trials performed and analyzed in the U.S. International Journal of Medical Sciences 2009; 6:143-155
Strobeck JE et al. A Paired-Comparison of the MultiFunction Cardiogram (MCG) and Sestamibi SPECT Myocardial Perfusion Imaging (MPI) to Quantitative Coronary Angiography for the Detection of Relevant Coronary Artery Obstruction (≥70%) - A Single-Center Study of 116 Consecutive Patients Referred for Coronary Angiography International Journal of Medical Sciences, 2011; 8(8): 717-724
John E. Strobeck, Norbert Rainford, Bonnie Arkus, and Michael Imhoff. Treatment Strategies (2010) Comparing Multifunction-Cardiogram and Coronary Angiography for Detection of Hemodynamically Relevant Coronary Artery Stenosis (>70%) in Women.
Amano T, Kunimura A, et al. Noninvasive assessment of functionally significant coronary stenoses through mathematical analysis of spectral ECG components. BMJ/Open Heart 2014;1:e000144. doi:10.1136/openhrt-2014-000144
Shinoda et al. Noninvasive Mathematical Analysis of Spectral Electrocardiographic Components for Coronary Lesions of Intermediate to Obstructive Stenosis Severity–Relationship with Classic and Functional SYNTAX Score. Catheterization and Cardiovascular Interventions DOI 10.1002/ ccd. Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI)
Tetsuya Amano, Norihiro Shinoda, et al. Impact of noninvasive mathematical analysis of spectral electrocardiographic components on predicting recurrent cardiac ischemic events after coronary intervention: An Abstract submitted for the 2015 PCI TCT in San Francisco.
Tetsuma Kawaji, MD; Hiroki Shiomi, MD; Takeshi Morimoto, MD, Ph.D.; Ryusuke Nishikawa, MD; Mariko Yano, MD; Hirooki Higami, MD; Junichi Tazaki, MD; Masao Imai, MD; Naritatsu Saito, MD; Takeru Makiyama, MD; Satoshi Shizuta, MD; Koh Ono, MD; and Takeshi Kimura, MD. Noninvasive Electrocardiology Journal (2015) Noninvasive Detection of Functional Myocardial Ischemia: Multifunction Cardiogram Evaluation in Diagnosis of Functional Coronary Ischemia Study (The “ED-HIT" Piece, perhaps?)
Michael Imhoff, MD, PhD; Norbert Rainford, MD. Noninvasive Electrocardiology Journal (2015). A Rebuttal Letter to the Editor: It All Depends on Your References: Electrophysiology Compared to Angiography.
A Japanese Style Retraction: (In Japanese only, translated) Validation of Multifunction CardioGram(MCG) in the screening of Coronary Atherosclerosis. Tetsuma Kawaji, MD; Hiroki Shiomi, MD; Takeshi Morimoto, MD, Ph.D.; Ryusuke Nishikawa, MD; Mariko Yano, MD; Hirooki Higami, MD; Junichi Tazaki, MD; Masao Imai, MD; Naritatsu Saito, MD; Takeru Makiyama, MD; Satoshi Shizuta, MD; Koh Ono, MD; and Takeshi Kimura, MD.
Access to ALL of the peer-reviewed published records in this historical journey: https://www.dropbox.com/sh/3n3k78hp454knkg/AAC75TMIP9WkTvPjAmGJH2Zda?dl=0
JJohn Ioannidis, “Most “esearch is Flawed; let’s let'st.” http”://www.medscape.com/viewarticle/898405
Marcia Angeles, the first woman editor-in-chief of the famous New England Journal of Medicine: https://www.bmj.com/rapid-response/2011/11/02/drug-companies-amp-doctors-story-corruption
Robert H. Lustig. METABOLICAL - ““he t"“““uth about processed food and how it
poisons people and the planet."" 2021 "“““https://robertlustig.com/metabolical/
The 56th Annual Scientific Meeting of the Japanese Ningen Dock Society Presentation and Announcement: https://www.dropbox.com/scl/fi/okspg3508b9sed7tae124/2016-56th-Annual-Scientific-Meeting-of-Japan-Society-of-Ningen-Dock.pdf?rlkey=cmiskm71x570x7cqmm9ucuq6d&dl=0
Japanese Ningen Dock Society has been credited with bringing better public health to Japan: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8884042/
Human Frailty is a Cash Cow: https://www.medscape.com/viewarticle/995726#vp_2?form=fpf
The first-generation work, including preclinical, phase I, and II human trials
Healthcare outcomes were assessed using observational study designs rather than randomized trials. Cochrane Database Syst Rev. April 29, 2014;2014(4): MR000034. Doi: 10.1002/14651858.MR000034.pub2.
Hi ALL,
I wish you and your families a delighted Holy Week, Good Friday, and Easter Weekend!
I've included updated clinical and technology due diligence material links below. They are comprehensive in design and should answer and satisfy most interested parties, even the most resistant and recalcitrant cardiologists:
This is Part I/III of the revised chapter published initially in Mark Houston’s Biomedical Textbook "Personalized and Precision Integrative Cardiovascular Medicine.” https://open.substack.com/pub/mcgdoc/p/the-cross-generationallifetime-work?r=q7iae&utm_campaign=post&utm_medium=web
Revised chapter part II/III, “The Journey to Freedom of a Recovered Physician,” describes our experience honestly and ethically conducting the independent third-party clinical validation without the business as usually corrupt “pay to play” schemes or without ANY quid pro quo: https://open.substack.com/pub/mcgdoc/p/the-journey-to-freedom-of-a-recovered?r=q7iae&utm_campaign=post&utm_medium=web
My DropBox Folder is organized to provide ALL the peer-review published papers and presentations performed by ourselves or by independent third parties: https://www.dropbox.com/sh/a9pg6te0ifn9o16/AAAVM-ZqeJbgs1E4kZJjgPyOa?dl=0
Two case reports demonstrating the unique capabilities of our technology to help patients with “Syndrome X” - the first, a retired ICU nurse who suffered repeated debilitating chest pains and tested “normal” on ALL her cardiology tests under the sun, then MCG came to her rescue: https://open.substack.com/pub/williamhbestermannjrmd/p/women-with-repeated-chest-pain-and-711?r=q7iae&utm_campaign=post&utm_medium=web; a 43-year-old overweight type two diabetic also who suffered repeated debilitating chest pains and tested “normal” on ALL his cardiology tests under the sun, then MCG came to his rescue: https://youtu.be/HvzVqtcRDdk
Our YouTube channel is created to educate and train customers: https://www.youtube.com/@premierheartllc7799
Thank you!
Joseph
“The limits of possible can only be defined by going beyond them into the impossible!”
Arthur C. Clark
Joseph T. Shen, a recovered physician,
Founded Computational BioCybernetics & Lagrangian Mechanics Systems Engineering Technologies
Researcher and Technology Developer
Managing Member
Premier Heart, LLC
Premier Heart International, LLC
Premier Heart Japan, Inc.
Emergency MCG USA, Inc.
110 Main Street, Suite 201-88
Port Washington, NY 11050
Tel: 516-883-3383 ex 8102
Fax: 516-883-5812
Mobile: 516-603-6368 (Please alert me who you are with a text message first; please do not respond to unknown numbers. I WILL respond as soon as possible.)
Email: jtshenmd@premierheart.com
The message is often dictated, so my apologies for the errors and typos.
IMPORTANT: This transmission is sent on behalf of Premier Heart, LLC; it may be privileged, proprietary, or confidential. It is intended only for the intended recipient. Suppose you are not the intended recipient or a person responsible for delivering this transmission to the intended recipient. In that case, you may not disclose, copy or distribute this transmission or take any action in reliance on it. If you received the communication in error, notify us immediately at (516) 883-3383 or by facsimile transmission at (516) 883-5812, and please dispose of and delete this transmission. Thank you.
I am thankful for your years of hard work and development. Am I certain mainstream physicians Find you very threatening. I always knew that was the case with alternative new ideas but after the past 3 years I am completely horrified by what I have seen. Your idea is a wonderful one and will save lives By helping people change their lifestyles before it's too late. But big pharma won't like that at all. Hang in there you are brave